Knowing when to resume sexual activity after an abortion matters for both your body and your emotions. This guide walks through practical timelines, how recovery differs after a medical versus a surgical abortion, and the possible risks of having sex too early. If you’re unsure about when it’s safe to be intimate again, this article is meant to offer clear, compassionate guidance — including emotional readiness and contraception options to help you feel safer and more prepared.
When Is It Safe to Resume Sex After an Abortion? General Guidelines and Timelines
Deciding when to have sex after an abortion comes down to how your body is healing and any individual risk factors. Most clinicians recommend waiting a set period to lower infection risk and let the cervix close, but the exact timing can vary depending on the procedure and your overall health.
What Is the Recommended Waiting Period Before Intercourse?
Most providers suggest waiting about one to two weeks before resuming intercourse. That window helps the cervix close and reduces infection risk. Some people may need a longer recovery if they have ongoing bleeding, pain, or other complications. Checking in with your healthcare provider is the best way to confirm what’s right for you.
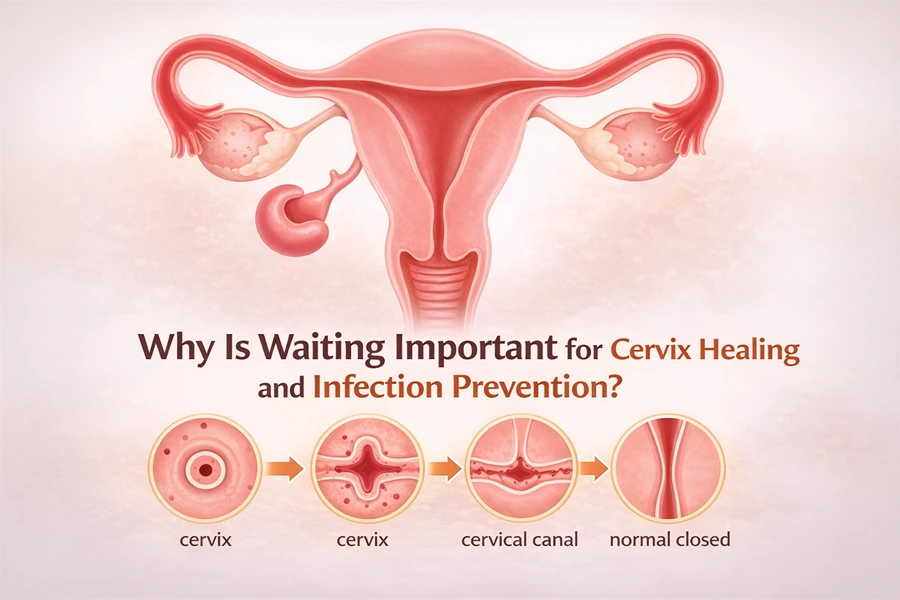
Why Is Waiting Important for Cervix Healing and Infection Prevention?
Waiting before sexual activity protects against several risks. The cervix can stay partially open for a short time after an abortion, which makes it easier for bacteria to enter the uterus. Having sex too soon can increase the chance of infection, heavier bleeding, or painful intercourse. Giving your body time to heal lowers those risks and helps make sex more comfortable when you’re ready.
How Does Recovery Differ Between Medical and Surgical Abortions? Specific Timelines for Resuming Sex
Recovery looks different after a medical abortion (the abortion pill) compared with a surgical procedure. Those differences can affect when it’s safe to resume sexual activity, so it helps to understand what each recovery typically involves.
When Can You Have Sex After a Medical Abortion or Abortion Pill?
After a medical abortion, most people are advised to wait at least one to two weeks before having sex. That gives time for the process to finish and for bleeding and cramping to settle. Pay attention to how you feel physically — if bleeding or pain continue, you may need more time and should follow up with your provider.
What Is the Safe Time for Intercourse After Surgical Abortion Procedures?
For surgical abortions, the usual recommendation is also about one to two weeks. Some people feel ready sooner, but it’s important to confirm healing with your clinician, especially if you had any complications. Trust your body’s signals and check in with your care team if you’re unsure.
What Are the Risks of Having Sex Too Soon After an Abortion? Infection and Other Health Concerns
Having sex before your body has healed can raise the risk of infection and other complications. Knowing what to watch for and how to reduce risk can help you make safer choices as you recover.
What Are the Signs of Infection to Watch For After Resuming Sex?
After you begin sexual activity again, be alert for signs that could indicate an infection:
Fever: A temperature above 100.4°F (38°C) may signal infection.
Unusual Discharge: Foul-smelling, greenish, or otherwise abnormal discharge is a warning sign.
Severe Pain: Intense pelvic pain that doesn't ease with over‑the‑counter medicine should be evaluated.
If you notice any of these symptoms, contact your healthcare provider promptly.
How Can You Reduce Infection Risk During Post-Abortion Sexual Activity?
To lower the chance of infection as you recover, consider these practical steps:
Wait the Recommended Time: Stick to the waiting period your provider suggests before having intercourse.
Practice Good Hygiene: Both partners should wash hands and genitals before sex to reduce bacterial transfer.
Use Protection: Condoms help protect against sexually transmitted infections and add an extra safety layer while you heal.
Following these precautions can make intimacy safer during the recovery period.
How Does Emotional Readiness Affect Resuming Sexual Activity After Abortion? Partner Communication and Psychological Aspects
Emotional readiness is as important as physical healing. Processing the experience and being honest with yourself and your partner can make a big difference in how comfortable intimacy feels afterward.
Why Is Emotional Recovery Important Before Having Sex Again?
Emotional healing gives you space to process feelings about the abortion and what intimacy will mean going forward. Jumping back into sex before you feel ready can trigger anxiety, guilt, or physical discomfort. Letting yourself recover emotionally often leads to healthier, more positive intimate experiences.
How Can You Talk to Your Partner About Resuming Intimacy?
Clear, compassionate conversation helps both partners feel safe. Try these approaches:
Be Honest: Share where you are emotionally and physically — what feels okay and what doesn’t.
Set Boundaries: Agree on what kinds of touch or activity feel comfortable and when to stop.
Listen Actively: Invite your partner to share their feelings and concerns without judgment.
Open dialogue builds trust and makes it easier to navigate intimacy at a pace that feels right for both of you.
What Contraception Options Should You Consider After an Abortion? Preventing Immediate Pregnancy
Because fertility can return quickly after an abortion, it’s wise to consider contraception soon after the procedure. Discussing options with your provider at follow‑up visits helps you choose a method that fits your needs.
When Should You Start Using Birth Control After Abortion?
It’s generally safe to start many forms of birth control immediately after an abortion, since fertility can return in as little as two weeks. Many clinicians recommend planning for contraception during your follow‑up appointment so you leave with a clear plan.
Which Contraceptive Methods Are Safe and Effective Post-Abortion?
Common, effective options you can typically use after an abortion include:
Hormonal Birth Control: Pills, patches, and injections can often be started right away.
Intrauterine Devices (IUDs): Both hormonal and copper IUDs can be inserted immediately after a surgical abortion or once bleeding has decreased after a medical abortion.
Barrier Methods: Condoms and diaphragms are usable immediately and also protect against STIs (condoms).
Which method is best depends on your preferences, medical history, and future plans — talk it over with your healthcare provider for personalized advice.
Method
Effectiveness
Notes
Hormonal Birth Control
91-99%
Requires consistent use
IUD (Hormonal)
99%
Long-term solution, can be used immediately after surgical abortion or when bleeding subsides after medical abortion
IUD (Copper)
99%
Non-hormonal option, can be used immediately after surgical abortion or when bleeding subsides after medical abortion
Condoms
85%
Protects against STIs, requires proper use
Frequently Asked Questions
What should I expect during the recovery process after an abortion?
Recovery varies from person to person. You may experience cramping, bleeding, and emotional ups and downs. Physically, most people recover over a few weeks, but emotional recovery can take longer. Keep an eye on any unusual symptoms and stay in touch with your healthcare provider for follow‑up care and reassurance.
Can I use tampons after an abortion?
Most providers recommend avoiding tampons for at least two weeks after an abortion to lower infection risk. Pads are a safer option during the initial recovery. As always, check with your clinician for guidance tailored to your situation.
How can I manage pain or discomfort after an abortion?
Over‑the‑counter pain relievers like ibuprofen or acetaminophen often help. A heating pad on the lower abdomen can ease cramps, and rest plus hydration supports recovery. If pain is severe or doesn’t improve, contact your healthcare provider.
What emotional support resources are available after an abortion?
Emotional support might include talking with trusted friends or family, counseling, support groups, or hotlines. Many reproductive health organizations offer resources and referrals. If feelings of anxiety, guilt, or sadness persist, reaching out to a professional can be very helpful.
Are there any lifestyle changes I should consider after an abortion?
Healthy habits support recovery: eat balanced meals, stay hydrated, and follow your provider’s advice about activity levels. Avoid smoking and limit alcohol while healing. Practices like gentle yoga, meditation, or breathing exercises can also help emotional recovery.
What should I do if I experience complications after an abortion?
If you have severe pain, heavy bleeding, fever, or other worrying symptoms, seek medical attention right away. Prompt care is important for treating complications, so keep your provider’s contact information handy during recovery.
Conclusion
Knowing when to resume sexual activity after an abortion helps protect your physical health and emotional well‑being. Follow the recommended waiting periods, listen to your body, and communicate openly with partners and healthcare providers. Prioritizing both physical healing and emotional readiness supports a safer, more comfortable return to intimacy. If you’d like more information or support, please explore our resources or contact a clinician you trust.
This article is for informational purposes only and does not constitute medical advice. It is not intended to replace professional medical evaluation, diagnosis, or treatment. Always consult a qualified healthcare provider with any questions about recovery, symptoms, or when it is safe to resume sexual activity after an abortion.
The abortion pill—also called medication abortion—is a safe, effective option for ending an early pregnancy. Knowing what it might cost helps you plan and find the right support. This guide explains the factors that affect price, the medications involved, typical cost ranges, and where to look for financial help. Because many people face money-related barriers to reproductive care, we walk through what to expect and how to prepare. Below you'll find plain explanations of: what the abortion pill is and how it works; average prices and ranges; what changes costs; financial help; telehealth versus in-person care; and what’s usually included in the total price.
What Is the Abortion Pill and How Does Medication Abortion Work?
The term “abortion pill” refers to a two-step medication regimen used to end an early pregnancy. It’s designed to be effective and to let many people complete the process in private. The two medicines most commonly used are mifepristone and misoprostol; together they safely end a pregnancy when used as directed.
What Are Mifepristone and Misoprostol?
Mifepristone is the first medicine in the regimen. It blocks progesterone, a hormone the pregnancy needs to continue, which causes the lining of the uterus to break down and the pregnancy to detach. Misoprostol is taken about 24–48 hours later to cause uterine contractions that expel the pregnancy tissue. Used together, these medications provide a medically proven option for early abortion.
How Is Medication Abortion Administered?
Medication abortion usually involves one or two visits with a medical provider. At the first visit you typically receive mifepristone and clear instructions for taking misoprostol at home. A follow-up appointment—either in person or remotely—is commonly scheduled within one to two weeks to confirm the process is complete and to answer any questions. Follow-up care helps ensure your health and safety throughout recovery.
What Are the Average Costs and Price Ranges for the Abortion Pill?
Costs for the abortion pill vary depending on provider type, where you live, and whether insurance contributes. Knowing common price ranges can help you budget and compare options.
What Is the National Median Price and Typical Cost Range?
Nationally, the median cost for a medication abortion generally falls between $300 and $800. Exact prices depend on the clinic, the services included, and local market factors—some places charge less, others more.
How Do Prices Vary by Provider, Including Planned Parenthood and Virtual Clinics?
Different providers can charge different amounts. Planned Parenthood clinics often offer medication abortion within the national median range. Some private clinics charge more, while virtual clinics may be less expensive because they have lower overhead. The table below shows typical ranges by provider type.
Provider Type
Average Cost Range
Planned Parenthood
$300 - $600
Private Clinics
$400 - $800
Virtual Clinics
$250 - $550
Which Factors Influence the Cost of the Abortion Pill?
Several variables affect the overall price. Understanding these can help you estimate costs and ask the right questions when you call a clinic.
How Does Gestational Age Affect Medication Abortion Pricing?
Gestational age is an important price driver. In general, earlier abortions tend to cost less. Medication abortion is typically offered up to 70 days (10 weeks) of pregnancy in the U.S.; as you approach that limit, care can become more complex and may cost more. You can read more about the cost of abortion in California.
How Do Location and State Laws Impact Abortion Pill Costs?
State rules and local regulations can increase cost. Requirements like mandatory counseling, waiting periods, or limits on telemedicine may add visits, travel, or administrative fees. Urban and rural differences in provider availability can also affect price and access.
What Role Does Insurance Coverage Play in Abortion Pill Affordability?
Insurance can significantly lower out-of-pocket costs, but coverage varies by plan and by state. Some plans cover medication abortion fully, others partially, and some not at all. Check with your insurer to learn what your policy covers and what you’ll owe.
What Additional Services Can Affect the Total Cost?
Extra services—like consultations, lab work, ultrasounds, or follow-up visits—may be billed separately and raise the total cost. Ask clinics for a complete price breakdown so you can plan for any additional fees.
How Can Financial Assistance Help Reduce Abortion Pill Costs?
Financial assistance can make medication abortion affordable for people who can’t cover the full price. A range of resources exists to help with procedure costs, travel, and related needs.
What Are Abortion Funds and How Can They Be Accessed?
Abortion funds are nonprofit organizations that provide grants and financial help to people seeking abortion care. They commonly assist with the cost of the procedure, travel, and other expenses. To access support, contact local or national abortion funds—many have simple application steps to determine eligibility.
How Do Sliding Scale Fees and Payment Options Work?
Many clinics use sliding scale fees based on income so people pay what they can afford. Some providers also offer payment plans or short-term financing. Ask the clinic about these options when you book an appointment.
How Do Telehealth and In-Person Abortion Pill Costs Compare?
Telehealth has expanded access and often changes the cost picture. Comparing telemedicine and in-person options can help you choose the approach that fits your needs and budget.
What Are the Benefits and Pricing Differences of Telemedicine Abortion?
Telemedicine for medication abortion is often more affordable, with typical prices ranging from $250 to $550. Remote visits reduce travel, time off work, and some facility fees, and can offer greater privacy and convenience for many people. For more information, read this guide on facts about medication abortion.
When Is In-Person Care Necessary and How Does It Affect Cost?
In-person care may be required for certain medical conditions, pregnancies beyond 10 weeks, or if you prefer face-to-face support. Clinic visits can cost more because they may include exams, facility fees, or additional services—but they also provide direct medical oversight and support.
What Should Be Included in the Abortion Pill Cost?
Knowing what is and isn’t included in a quoted price helps you avoid surprises and ensures you get complete care.
Which Medications and Services Are Usually Covered?
Quoted costs commonly cover both mifepristone and misoprostol and may include the initial consultation and at least one follow-up. Confirm with your provider which specific services are part of the price before you book.
What Additional Costs Might Patients Expect?
Additional charges can come from required lab tests, ultrasounds, or extra follow-up care. Talk through potential fees with your clinic so you know the full financial picture before moving forward.
Frequently Asked Questions
What is the difference between medication abortion and surgical abortion?
Medication abortion uses pills to end an early pregnancy and is usually available up to about 10 weeks. It lets many people complete the process at home. Surgical abortion is a clinic procedure to remove the pregnancy and is used later in pregnancy or when medication abortion isn’t appropriate. Both are safe when provided by trained clinicians; your provider can help you choose the best option for your situation.
Are there age restrictions for obtaining the abortion pill?
There are no federal age limits for the abortion pill, but state laws vary. Some states require parental consent or notification for minors. If you’re under 18, check your state’s rules and talk with a trusted adult or a healthcare provider—many clinics can explain local requirements and support you.
Can I use the abortion pill if I have certain medical conditions?
Most people can safely have a medication abortion, but some health conditions—like an ectopic pregnancy, severe anemia, or certain bleeding disorders—may make it unsafe. Always discuss your health history with a provider so they can recommend the safest option for you.
What should I expect during the medication abortion process?
Medication abortion commonly involves two visits. At the first visit you receive mifepristone and instructions for taking misoprostol at home. After misoprostol you can expect cramping and bleeding as your body expels the pregnancy. A follow-up visit confirms the abortion is complete. Arrange for support and contact your provider if you have heavy bleeding, fever, or other concerning symptoms.
How can I find a provider for the abortion pill?
You can find providers through Her Smart Choice, local reproductive health clinics, and telehealth services. Online directories, hotlines, and community organizations also help connect people to care. Choose a reputable clinic that offers clear information, confidentiality, and follow-up support.
What are the potential side effects of the abortion pill?
Common side effects include cramping, bleeding, nausea, vomiting, diarrhea, and tiredness—these are signs the medication is working. In rare cases people may experience heavy bleeding or infection. Monitor your symptoms and contact your healthcare provider if you’re worried or if symptoms are severe. Follow-up care is important to make sure you’ve recovered fully.
Conclusion
Knowing what the abortion pill may cost helps you make clearer, safer choices about your care. By reviewing typical prices, cost drivers, and financial support options, you can better plan and find the resources you need. If you have questions or need help, reach out to local clinics, abortion funds, or trusted healthcare professionals. Explore our other guides and contact providers to get the support and information that fit your situation.
Sexually transmitted diseases remain common in the United States, and many women experience barriers to timely care. According to the CDC, millions of new STD cases are diagnosed each year, and many infections cause mild or no symptoms in women. That gap between exposure and diagnosis can lead to complications that affect fertility, pregnancy outcomes, and long-term health. Telehealth has emerged as a practical way to close that gap by offering private consultations, convenient testing options, and treatment guidance without the need for an in-person visit.
Telehealth services for STD consultations connect patients with licensed clinicians through secure video or messaging platforms. For women, these services can offer discretion, flexible scheduling, and access to care even when local clinics are difficult to reach. This article explains what telehealth STD services are, how they work, and how to evaluate the best options for women. It also covers testing, treatment, safety considerations, and when in-person care is still necessary.
What is telehealth for STD consultations?
Telehealth for STD consultations refers to medical care delivered remotely for concerns related to sexually transmitted infections. This typically includes symptom assessment, sexual health counseling, ordering laboratory tests, reviewing results, and prescribing treatment when appropriate. Services are provided by licensed clinicians who follow state and federal regulations.
During a telehealth visit, a clinician reviews symptoms, sexual history, and risk factors. If testing is needed, the clinician may order lab work at a nearby facility or arrange an at-home collection kit when available. Results are reviewed with the patient, and treatment or follow-up care is discussed. Telehealth does not replace all in-person services, but it can be an effective first step for many women seeking STD evaluation.
Telehealth STD services are often confused with online test ordering sites. The key difference is clinical oversight. A true telehealth consultation includes a medical evaluation and guidance from a licensed provider rather than test ordering alone.
Why telehealth can be a strong option for women
Women face unique challenges related to sexual health. Many STDs are asymptomatic in women, which can delay diagnosis. Others cause symptoms that overlap with common gynecologic conditions. Telehealth can help address these challenges in several ways.
Privacy and discretion are major benefits. Telehealth visits can be completed from home, reducing concerns about stigma or visibility at a clinic. Convenience is another advantage, especially for women balancing work, caregiving, or limited transportation. Telehealth may also improve access for women in areas with few women’s health clinics.
Telehealth services can complement care from a women’s health clinic by offering faster initial assessment and follow-up discussions. Some women use telehealth as their primary entry point into care, while others use it between in-person visits.
Common STDs addressed through telehealth
Most telehealth STD services focus on common infections that can be evaluated and managed remotely in many cases.
Chlamydia and gonorrhea
Chlamydia and gonorrhea are among the most frequently reported bacterial STDs in the United States. Many women have no symptoms. When symptoms occur, they may include abnormal discharge, pelvic pain, or pain during urination. Telehealth clinicians can assess risk and order testing. According to CDC guidelines, these infections are treatable with antibiotics once confirmed.
Human papillomavirus
HPV is very common and often clears on its own. Some strains are linked to cervical cancer. Telehealth clinicians can provide education, discuss screening schedules such as Pap tests, and guide follow-up care. HPV testing itself is usually performed during in-person cervical screening, but telehealth can support counseling and prevention.
Genital herpes
Herpes simplex virus causes recurrent outbreaks of sores or blisters. Diagnosis may be based on symptoms, history, and testing. Telehealth clinicians can discuss suppressive or episodic antiviral therapy. Research published in the New England Journal of Medicine shows that antiviral treatment can reduce outbreak severity and transmission risk.
Syphilis
Syphilis progresses through stages and can cause serious complications if untreated. Telehealth can help with risk assessment and ordering blood tests. Treatment typically requires in-person administration of medication, so telehealth often serves as an initial step rather than complete care.
HIV
HIV testing and counseling are essential components of sexual health. Telehealth services can provide pre-test counseling, order testing, and discuss results. Ongoing HIV management usually requires in-person care, but telehealth can support education and linkage to services.
How telehealth STD consultations work
Understanding the typical process can help women choose the right service.
Initial consultation
The visit usually begins with a detailed medical and sexual history. Clinicians ask about symptoms, recent exposures, contraceptive use, and pregnancy status. This information helps determine testing needs and urgency.
Results are reviewed during a follow-up telehealth visit or through secure messaging. Clinicians explain what the results mean and discuss next steps. If treatment is indicated and permitted by state law, prescriptions may be sent to a local pharmacy.
Treatment and counseling
Treatment plans follow established guidelines such as those from the CDC. Clinicians also provide counseling on partner notification, prevention, and follow-up testing when needed.
What to look for in the best telehealth STD services
Not all telehealth services are the same. Several factors can help identify high-quality options.
Licensed clinicians and credentials
The service should clearly state that care is provided by licensed physicians, nurse practitioners, or physician assistants. Providers should be licensed in the patient’s state, which is required for telehealth care in the United States.
Evidence-based care
Best services follow current clinical guidelines. They explain testing accuracy, treatment effectiveness, and limitations. According to the CDC, adherence to evidence-based protocols is essential for STD management.
Clear testing pathways
High-quality services explain how testing is done, where samples are collected, and how results are delivered. They also clarify what infections can and cannot be managed remotely.
Privacy and data security
Telehealth platforms should use secure systems that protect patient information. Women should be able to review privacy policies and understand how data is stored and shared.
Integration with women’s health needs
Some services take a broader approach to reproductive and sexual health. A women-focused clinic such as Her Smart Choice may integrate STD consultations with counseling on contraception, pregnancy considerations, and access to in-person care when needed. This integrated approach can be helpful for women who want continuity across different aspects of care.
Telehealth versus in-person women’s health clinics
Telehealth and in-person clinics each play an important role in women’s healthcare. Virtual visits can make it easier to access care quickly, while in-person clinics remain essential for exams and hands-on treatments. For many women, using both options offers the most comprehensive support.
Telehealth may be appropriate for initial assessment, routine screening discussions, and treatment of uncomplicated infections. In-person care is necessary for pelvic exams, certain tests, injections, and management of complications. Cleveland Clinic experts note that combining remote and in-person care can improve access without compromising safety.
Treatment options available through telehealth
Treatment depends on the infection and individual circumstances.
Antibiotic therapy
For bacterial STDs such as chlamydia and gonorrhea, telehealth clinicians can prescribe antibiotics once testing confirms the diagnosis. The CDC regularly updates recommended regimens based on resistance patterns.
Antiviral therapy
For herpes, antiviral medications may be prescribed to reduce symptoms and transmission risk. Treatment plans are individualized based on outbreak frequency and patient preferences.
Supportive care and counseling
Education on prevention, condom use, and partner testing is a core part of care. Telehealth clinicians often spend time addressing questions and concerns that may not be fully covered during brief clinic visits.
Prevention and screening considerations for women
Prevention is a key component of sexual health.
Regular screening
CDC recommendations include routine screening for chlamydia and gonorrhea in sexually active women under 25 and in older women with risk factors. Telehealth can support scheduling and follow-up.
Vaccination
HPV vaccination is recommended for many adolescents and young adults. Telehealth clinicians can provide guidance on eligibility and direct patients to vaccination sites.
Risk reduction strategies
Counseling on barrier methods, communication with partners, and testing frequency is part of comprehensive care. Research published in JAMA suggests that counseling combined with testing improves prevention outcomes.
Living with an STD and ongoing care
An STD diagnosis can be emotionally challenging. Telehealth services can provide ongoing support, education, and follow-up. For chronic conditions such as herpes or HIV, coordination with in-person providers is important. Prognosis varies by condition, but early diagnosis and adherence to treatment are associated with better outcomes.
Women should plan regular follow-up and discuss future reproductive goals with their healthcare providers. Telehealth can help maintain continuity, especially between clinic visits.
FAQs
How accurate is STD testing ordered through telehealth?
Accuracy depends on the type of test and sample collection. Laboratory-based tests ordered through telehealth follow the same standards as in-person orders. According to the CDC, nucleic acid amplification tests used for chlamydia and gonorrhea are highly sensitive and specific when collected correctly.
Can telehealth doctors prescribe treatment for STDs?
In many cases, yes. Licensed clinicians can prescribe medications for certain STDs after appropriate evaluation and testing, as allowed by state law. Some treatments still require in-person administration, which the clinician will explain.
Is telehealth safe for STD care during pregnancy?
Telehealth can be used for counseling and initial assessment during pregnancy, but testing and treatment decisions require careful coordination with obstetric care. The CDC recommends prompt evaluation of STDs in pregnancy due to potential risks to both mother and baby.
What symptoms should prompt immediate in-person care?
Severe pelvic pain, fever, heavy bleeding, or symptoms of advanced infection require urgent in-person evaluation. Telehealth clinicians will advise when symptoms suggest complications that cannot be managed remotely.
How private are telehealth STD services?
Reputable services use secure platforms to protect patient information. Privacy policies should clearly explain data handling. Many women choose telehealth specifically for its discretion compared to waiting rooms.
Can telehealth replace a women’s health clinic completely?
Telehealth can handle many aspects of STD care, but it does not replace physical exams and procedures. Most experts recommend using telehealth alongside regular in-person care for comprehensive women’s health.
How do I choose between different telehealth providers?
Look for licensed clinicians, evidence-based protocols, clear testing options, and transparent privacy practices. Women-focused services that integrate reproductive health, such as Her Smart Choice, may offer added continuity for some patients.
Medical Disclaimer and Conclusion
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider for diagnosis and treatment.
Telehealth has become an important tool for STD consultations, especially for women seeking privacy, convenience, and timely care. High-quality services provide licensed clinicians, evidence-based testing, and clear follow-up pathways. Telehealth works best when combined with appropriate in-person care and regular screening. By understanding how these services work and what to look for, women can make informed choices that support their sexual and reproductive health.
Sexually transmitted infections (STIs), commonly called sexually transmitted diseases (STDs), are infections most often passed during sexual contact that can affect the reproductive system and overall health. This guide walks you through what STIs/SDs are, why clinicians distinguish “infection” from “disease,” how common STIs typically show up in women, and the clinical risks they pose for fertility and abortion care. You’ll get clear explanations of how chlamydia, gonorrhea, syphilis, herpes, HPV, trichomoniasis, and HIV behave biologically, which signs to watch for, and why routine screening matters even when there are no symptoms. We also cover testing methods, treatment strategies (curative versus suppressive), practical prevention steps like condoms and vaccination, and the reasons testing is often recommended before abortion procedures. Finally, find compassionate next steps for people seeking care or counseling.
STDs and STIs: What They Mean, How They Differ, and the Most Common Types
An STI (sexually transmitted infection) means a pathogen—bacteria, virus, or parasite—has colonized genital, oral, or rectal mucosa. An STD (sexually transmitted disease) refers to when that infection causes symptoms or tissue damage. Clinicians prefer “STI” to emphasize catching infections early and preventing disease, though both terms are used in everyday conversation. Knowing whether an infection is bacterial, viral, or parasitic helps predict which conditions are curable and which require ongoing management, and it explains why screening approaches vary by pathogen. Finding infections early lowers the chance of complications and stops onward spread by allowing timely treatment or suppression—an important safeguard for reproductive health. Below are the most commonly referenced STIs in clinical guidance and public health materials.
Common STIs include:
Chlamydia: A bacterial infection that’s often silent in women but curable with antibiotics.
Gonorrhea: A bacterial infection that can cause abnormal discharge and pelvic pain; rising antibiotic resistance makes quick treatment essential.
Syphilis: A systemic bacterial infection that progresses in stages and can cause serious long-term harm if untreated.
Herpes (HSV): A viral infection that causes periodic genital sores and is managed with antiviral medications.
Human papillomavirus (HPV): A group of viruses that can cause genital warts and, for certain types, cervical changes that may lead to cancer; vaccines prevent the highest-risk strains.
Trichomoniasis: A parasitic infection that commonly causes discharge and irritation and is curable with antiparasitic treatment.
HIV: A virus that attacks the immune system and requires lifelong antiretroviral therapy.
This quick list helps clarify pathogen type, how infections spread, and whether they’re curable.
Infection
Pathogen Type / Transmission
Curable?
Chlamydia
Bacteria — sexual genital/rectal exposure
Yes (antibiotics)
Gonorrhea
Bacteria — sexual genital/rectal/oral exposure
Yes (antibiotics; resistance concerns)
Syphilis
Bacteria — sexual contact, can be systemic
Yes (antibiotics when treated early)
Herpes (HSV)
Virus — skin/mucosal contact during outbreaks or asymptomatic shedding
No (manageable with antivirals)
HPV
Virus — skin/mucosal contact; some types oncogenic
No (infections may clear on their own; vaccine prevents high‑risk types)
Trichomoniasis
Parasite — vaginal sexual exposure
Yes (antiparasitic treatment)
HIV
Virus — blood, sexual contact, vertical transmission
No (lifelong management with antiretrovirals)
Infection vs. Disease: Understanding Medical Terms and Common Synonyms
In medical language, “infection” means a germ is present; “disease” means that presence is causing symptoms or measurable harm. That difference matters because many STIs don’t cause noticeable symptoms—an infection can be silent—so screening lets clinicians treat infections before they become disease. Public health groups often use the term “STI” to reduce stigma and focus on prevention. For example, a positive nucleic acid amplification test (NAAT) shows an STI even if someone feels fine. Clinicians explain these terms to help patients understand why treatment or partner notification may be advised even without symptoms.
Seeing this distinction makes the case for screening: if infections are frequently silent, proactive testing and early treatment are key to protecting reproductive health and preventing complications like pelvic inflammatory disease. The next section lays out the main pathogen categories with examples to make these concepts concrete.
Main Types of STIs: Bacterial, Viral, and Parasitic Infections
Practically speaking, STIs fall into three categories—bacterial, viral, and parasitic—each with different implications for care. Bacterial STIs such as chlamydia, gonorrhea, and syphilis are usually curable with antibiotics, so early detection can prevent long-term reproductive damage. Viral STIs like herpes, HPV, and HIV are generally managed rather than cured: antivirals can suppress symptoms and lower transmission risk, while vaccination prevents many HPV-related cancers. Parasitic infections—most commonly trichomoniasis—are treated effectively with antiparasitic medications and often cause characteristic discharge and irritation.
Bacterial STIs: Chlamydia, gonorrhea, syphilis — often curable with antibiotics.
Viral STIs: Herpes (HSV), HPV, HIV — managed with antivirals and prevented in part by vaccines (HPV) or prophylaxis.
Parasitic STIs: Trichomoniasis — curable with antiparasitic medication.
Knowing these categories helps patients and clinicians pick the right tests, follow-up care, and partner treatment or vaccination when appropriate.
Common STD Symptoms in Women: Early Signs and Silent Infections
STIs in women can cause symptoms in the vulva, vagina, cervix, urinary tract, and, less commonly, systemically. Many infections, however, are asymptomatic and only found through screening. Typical symptoms include abnormal vaginal discharge that varies in color and consistency, pelvic or lower abdominal pain that may indicate upper genital tract involvement, painful or frequent urination, and localized sores or lesions. Because symptoms overlap between infections, clinicians usually rely on targeted testing rather than diagnosis by symptoms alone. Spotting symptoms early supports prompt testing, treatment, and interruption of transmission.
Warning signs in women that suggest an STI include:
Abnormal vaginal discharge — yellow, green, frothy, or unusually smelly compared with your normal baseline.
Pelvic or lower abdominal pain, especially when paired with fever or pain after sex.
Painful urination or increased urinary frequency, which can mimic a urinary tract infection.
Genital sores, blisters, or ulcers, which may indicate herpes, syphilis, or other causes.
When these signs occur, clinicians typically perform a pelvic exam, collect swabs for NAAT testing, and order blood tests as needed; early diagnosis allows quick antibiotic or antiviral treatment and lowers the chance of complications. Prompt evaluation also makes partner notification and treatment possible, which reduces reinfection and community spread.
Which Symptoms Point to an STD in Women: Discharge, Pain, and Sores
Certain symptom patterns can suggest likely infections but aren’t definitive without testing. A mucopurulent or yellow‑green discharge often suggests chlamydia or gonorrhea, while frothy green discharge is more typical of trichomoniasis; clear, watery discharge may be non‑infectious. Pelvic or lower abdominal pain—especially with fever or cervical motion tenderness—raises concern for pelvic inflammatory disease (PID), commonly a complication of untreated chlamydia or gonorrhea. Genital sores or ulcers can signal herpes simplex or primary syphilis and usually require lesion swabs and blood tests for an accurate diagnosis.
Because symptoms overlap and some infections are silent, a low threshold for testing is the safest approach: if infection is suspected or routine screening is due, clinicians collect targeted samples and order the most sensitive tests for the likely pathogens. Early detection and treatment prevent progression and decrease transmission to partners.
Why Many STIs Are Asymptomatic in Women and What That Means for Detection
Several biological factors explain why many STIs are silent in women: infections often sit on mucosal surfaces, provoke a lower inflammatory response, and shed intermittently. Hormonal influences and the anatomy of the female reproductive tract can allow pathogens to persist without noticeable symptoms, while partner infections can go unrecognized. This silent course makes routine screening especially important to catch infections before they ascend to the upper genital tract and cause PID, infertility, or ectopic pregnancy.
Screening guidelines prioritize testing sexually active women under certain ages or with risk factors and emphasize NAAT-based urine or vaginal swab testing for chlamydia and gonorrhea because these methods detect infection even when there are no symptoms. Regular screening, timely treatment, and partner management together reduce the public-health burden of undiagnosed infections.
How STIs Affect Female Reproductive Health and Fertility
Untreated STIs can directly damage reproductive organs, trigger chronic inflammation, and raise the risk of adverse pregnancy outcomes—so prevention and early treatment are essential for preserving fertility. When infections move up from the cervix into the uterus and fallopian tubes, they can cause pelvic inflammatory disease (PID), leading to scarring, tubal blockage, and higher risk of infertility or ectopic pregnancy. Persistent infection with high‑risk HPV types can lead to cervical dysplasia and, over time, cancer, highlighting the importance of vaccination and regular screening. Understanding these mechanisms shows why screening and prompt treatment protect more than just immediate symptoms.
Cervical cancer: Persistent high‑risk HPV infection can lead to precancerous changes and cancer.
These outcomes explain why clinicians stress screening and timely treatment: stopping infection before it causes structural damage helps preserve reproductive potential and lowers obstetric risks.
What Is Pelvic Inflammatory Disease and How Is It Linked to Untreated STIs?
Pelvic inflammatory disease (PID) is inflammation of the upper reproductive tract—uterus, fallopian tubes, and ovaries—most often caused by untreated cervical infections like chlamydia and gonorrhea that ascend into the tubes. PID typically presents with lower abdominal pain, fever, abnormal bleeding, and cervical motion tenderness; diagnosis rests on clinical criteria supported by lab testing and sometimes imaging. The inflammatory process and subsequent scarring in the fallopian tubes are the main pathways by which PID leads to infertility and ectopic pregnancy. Prompt antibiotic treatment and follow-up reduce the risk of lasting damage, but repeated PID episodes raise cumulative risk.
Recognizing early PID signs and testing for common bacterial causes are essential steps to interrupt this disease process and protect future fertility.
How STIs Can Lead to Infertility, Ectopic Pregnancy, and Cervical Cancer
Different pathogens carry different long‑term risks: chlamydia and gonorrhea are strongly linked to tubal scarring that can cause infertility and ectopic pregnancy, while persistent infection with oncogenic HPV types is the main cause of cervical cancer. Chronic inflammation from untreated infections damages epithelial tissue and promotes fibrotic repair that narrows or blocks fallopian tubes, disrupting fertilization and embryo transport. HPV drives cellular changes through viral oncogenes, a process preventable with vaccination and detectable with routine cervical screening. Early detection, timely antibiotic or antiviral therapy, and vaccination together lower the population risk of these serious reproductive outcomes.
Using vaccination, regular screening, and prompt treatment together creates a layered defense that helps preserve fertility and reduce cancer risk over a lifetime.
Why STI Testing Matters Before Abortion Care
Testing for STIs before abortion care matters because untreated infections can raise the risk of procedural complications, postoperative infection, and pelvic inflammatory disease—issues that can affect healing and future fertility. If an STI is identified before a medical or surgical abortion, clinicians can start treatment or adjust procedural plans to reduce infection‑related risks. Rapid tests—like NAATs on urine or vaginal swabs and point‑of‑care syphilis or HIV tests—help clinicians make timely decisions before intervention. For people seeking abortion care, confirming STI status is part of comprehensive reproductive care that protects both immediate outcomes and long‑term reproductive health.
Comparison of tests commonly used for pre‑procedure screening:
Test Type
Sample Used / Turnaround
When Recommended
NAAT (chlamydia/gonorrhea)
Urine or vaginal swab — results often within 24–72 hours
Routine pre‑procedure screening for sexually active patients
Blood serology (syphilis, HIV)
Blood sample — rapid tests available; standard serology may take days
Recommended before invasive procedures or when risk factors are present
Lesion swab (HSV)
Swab from sore — PCR available with variable turnaround
When genital lesions are present at evaluation
Wet mount / microscopy (trichomonas)
Vaginal swab — immediate on‑site results possible
For symptomatic discharge or in limited‑resource settings
Risks of Untreated STIs During Abortion Procedures
Having an untreated STI at the time of an abortion can increase the chance of post‑procedural infection and PID, which can complicate recovery and raise the risk of longer‑term reproductive harm. For example, an ascending chlamydial or gonococcal infection around the time of instrumentation may trigger a stronger inflammatory response, higher fever, and a greater need for extended antibiotics or hospitalization. The level of procedural risk depends on the abortion method (medical versus surgical) and the infection involved, but the consistent clinical approach is to test and treat identified infections before or soon after the procedure to reduce complications. Clear patient education about testing timelines and rapid access to results are practical steps that help lower risk and improve outcomes.
Timely screening, same‑day testing when available, and prompt initiation of therapy when infections are detected are key clinical strategies to protect patients undergoing abortion care.
How Her Smart Choice Supports Accessible STI Testing and Counseling
Search results describe Her Smart Choice as a provider of comprehensive women’s health services, including STI testing and treatment alongside abortion care. Unique value points highlighted include clear, compassionate guidance on sexual and reproductive health; emphasis on testing and treatment before or after abortion care to reduce PID and infertility risk; and accessible services such as same‑day appointments and possible low‑cost or free options for people with financial need.
Her Smart Choice combines confidential counseling with testing pathways that prioritize same‑day access and patient-centered education, so people understand testing choices and the clinical reasons for pre‑procedure screening. Clinical decisions remain evidence‑based and individualized, but pairing counseling, rapid testing, and coordinated treatment reduces logistical barriers that can delay care. Patients are encouraged to discuss testing timing relative to their procedure and to ask about financial or support resources; early testing and partner notification are practical steps to limit complications and protect reproductive health.
These service features create a supportive clinical experience where prevention strategies are matched with practical access measures to reduce STI‑related risks around abortion care.
Effective STI Treatment and Prevention Strategies
Managing STIs effectively combines curative antibiotics for most bacterial and parasitic infections, suppression strategies for viral infections, and prevention measures like condoms and vaccination to reduce transmission and long‑term harm. Bacterial infections—chlamydia, gonorrhea, syphilis—are usually treatable with appropriate antibiotics, so prompt diagnosis is highly effective at preventing complications. Viral infections such as herpes and HIV are managed with antivirals to reduce symptoms and transmissibility; HPV prevention relies heavily on vaccination to block high‑risk types that cause cervical cancer. Prevention also includes regular screening, consistent condom use, reducing the number of sexual partners, and quick partner notification and treatment when infections are found.
Infection
Standard Treatment
Vaccine Available
Partner Treatment Needed
Chlamydia
Antibiotics (curative)
No
Yes (to prevent reinfection)
Gonorrhea
Antibiotics (curative; monitor resistance)
No
Yes
Syphilis
Antibiotics (curative if early)
No
Yes
Herpes (HSV)
Antivirals (suppressive, not curative)
No
Partner counseling recommended
HPV
Management of lesions; vaccination prevents
Yes (prevents common oncogenic types)
Vaccination recommended for eligible partners
Trichomoniasis
Antiparasitic/antibiotic (curative)
No
Yes
This table contrasts cure versus suppression goals and underscores partner treatment and vaccination as central prevention tools.
If you need local testing, treatment, or follow‑up support, connecting with clinics that offer testing, counseling, and same‑day appointments improves timely care. Search results describe Her Smart Choice as a comprehensive provider of women’s health services, including STI testing and treatment and abortion care, with value points like compassionate guidance, pre‑ and post‑procedure testing/treatment to reduce PID and infertility, and accessible appointment options for people with limited resources.
Which Treatments Cure or Manage Common STIs: Antibiotics and Antivirals
Antibiotics can cure most bacterial STIs by eradicating the organisms, preventing progression to complications when given promptly and correctly. Antivirals do not remove latent viral genetic material but reduce outbreak frequency and severity and lower transmission risk—for example, long‑term antiviral suppression for herpes can improve quality of life and reduce viral shedding. HPV is best prevented by vaccination, which dramatically lowers rates of cervical dysplasia, while existing lesions are managed clinically. Treating partners and adopting safer behaviors are key complements to medication because untreated partners can cause reinfection.
These treatment principles emphasize that curable infections need prompt antibiotic therapy and that viral infections are managed with suppression and prevention strategies—reasons why testing and partner management are integral to effective care.
How Condoms, Vaccination, and Behavior Change Reduce STI Transmission
Barrier methods like condoms substantially lower the chance of transmitting many STIs by blocking contact with infectious fluids and affected skin. Consistent, correct condom use reduces risk for HIV, chlamydia, gonorrhea, and trichomoniasis and decreases HPV exposure. Vaccination—especially the HPV vaccine—is a powerful prevention measure that protects against the strains most linked to cervical and other anogenital cancers. Behavioral strategies such as limiting concurrent partners, keeping up with regular screening, and treating detected infections promptly further reduce community transmission and individual risk. Using behavioral, barrier, and biomedical approaches together creates the most robust protection against STIs.
Talk with your provider about vaccination eligibility and how often you should be screened so your prevention plan matches your needs. Education and easy access to services are essential to improving vaccine uptake and lowering long‑term disease burden.
Search results describe Her Smart Choice as a provider of comprehensive women's health services, including STI testing and treatment and abortion care. Key value points include compassionate education about sexual health, emphasis on testing and treatment to prevent PID and infertility around abortion care, and accessible options like same‑day appointments or low‑cost services for those in need.
In short: integrated clinical services—testing, counseling, vaccination, and treatment—work together to prevent complications and preserve reproductive health. If you have symptoms, a recent exposure, or an upcoming procedure, seek testing promptly and ask about counseling and treatment options to protect your health and fertility.
Frequently Asked Questions
1. What are the long-term effects of untreated STIs on women's health?
Untreated STIs can lead to serious long‑term problems for women, including pelvic inflammatory disease (PID), infertility, and ectopic pregnancy. PID can scar reproductive organs and interfere with fertility, and persistent infections like high‑risk HPV can progress to cervical cancer. Regular screening and prompt treatment are key to preventing these outcomes and protecting reproductive health.
2. How often should women get tested for STIs?
At minimum, sexually active women should be tested at least once a year, and more often if they have new or multiple partners or other risk factors. Women under 25 are especially encouraged to have annual screenings for chlamydia and gonorrhea. More frequent testing may be appropriate based on sexual activity and clinical guidance. Regular screening helps catch infections early—even when there are no symptoms—and lowers the chance of complications.
3. Can STIs affect pregnancy outcomes?
Yes. STIs such as chlamydia and gonorrhea can increase the risk of preterm labor, low birth weight, miscarriage, and transmission of infection to the baby during delivery. Treating STIs during pregnancy is important to protect both the parent and the newborn. Pregnant people should be screened and treated according to current clinical recommendations.
4. What is the role of partner notification in STI management?
Partner notification is an important part of STI control. Letting recent sexual partners know about an exposure enables them to get tested and treated, reducing reinfection risk and stopping further spread. Many providers offer confidential resources and support to help patients notify partners safely and effectively.
5. Are there any vaccines available for STIs?
Yes. The HPV vaccine protects against the strains most likely to cause cervical cancer and genital warts, and the hepatitis B vaccine prevents hepatitis B virus infection. Vaccination is a powerful preventive tool that reduces the burden of these infections and their complications.
6. How can lifestyle changes help prevent STIs?
Simple lifestyle steps can lower STI risk: use condoms consistently and correctly, reduce the number of sexual partners, and have open conversations about sexual health with partners. Regular health checkups and testing, as well as maintaining overall health through good nutrition and exercise, also help support immune function and early detection.
7. What should I do if I suspect I have an STI?
If you think you might have an STI, seek medical care promptly. Schedule testing and avoid sexual contact until you’ve been evaluated and treated if needed. Be honest with your healthcare provider about symptoms and sexual history so they can recommend the right tests and treatment. Early diagnosis and treatment make management more effective and reduce the chance of complications.
Conclusion
Knowing how STIs affect women’s reproductive health helps you take practical steps to prevent and treat infections early. Regular screening and timely treatment greatly reduce the risks of infertility and pelvic inflammatory disease. By prioritizing sexual health, seeking care when needed, and using prevention tools like condoms and vaccination, you can protect your reproductive future. Explore our resources and book a test today to take the next step in safeguarding your health.
Spotting on birth control — often called breakthrough bleeding — means light vaginal bleeding or brown discharge that appears between expected periods or instead of a full flow. It’s a common response to changes in hormonal contraception. This article breaks down what spotting looks like, the biology behind it, how often it happens with different methods, when it’s usually harmless, and when to seek medical care. If spotting feels worrying or lasts longer than you'd expect, Her Smart Choice offers supportive, non-promotional guidance and care navigation to help you decide if a clinical evaluation is needed. Many people go through an adjustment phase in the first months after starting or switching methods; knowing typical timelines, common causes, and practical steps can ease anxiety and help keep contraception effective. Below you’ll find clear definitions, cause-and-effect explanations, method-by-method comparisons, red-flag signs, practical ways to reduce spotting, and a description of how Her Smart Choice can support you with personalized reproductive health questions.
Is Spotting on Birth Control Normal? Understanding Breakthrough Bleeding
Spotting — medically called breakthrough bleeding — is most often a harmless response to hormonal shifts from contraception and usually improves within about three to six months after starting or changing a method. It happens because the uterine lining (the endometrium) becomes unstable when hormone levels fluctuate or when progestin is dominant, causing light, irregular bleeding rather than a full menstrual bleed. When contraception is used correctly, spotting rarely means the method has failed; however, bleeding that continues beyond the typical adjustment window or occurs with “red-flag” symptoms should be checked. Current guidance (as of 2024) notes that many low-dose and progestin-only regimens produce transient spotting while the body adapts, and clinicians often recommend observing for a few cycles before making changes. This section explains what spotting usually looks like and how common it is so you know what to expect.
How spotting usually differs from a period:
Light brown or pink staining rather than a steady bright red flow that needs protection.
Short, intermittent episodes lasting hours to a few days instead of the 3–7 days of a typical period.
Irregular timing — often outside the withdrawal-bleed window for combined pills.
What is Spotting and How Does It Differ from Menstrual Bleeding?
Spotting is usually scant bleeding or brown discharge that reflects older blood. A menstrual period is a coordinated shedding of the full uterine lining and shows as a heavier, brighter red flow. Mechanistically, spotting comes from localized endometrial instability or minor surface shedding, while a period follows a predictable hormonal withdrawal that causes a more complete lining breakdown. In practice, spotting rarely soaks a pad or tampon and often appears as a few drops or light staining in underwear; it can be intermittent and unpredictable. Recognizing these visual and timing differences helps you tell harmless breakthrough bleeding apart from heavier or abnormal bleeding that may need evaluation.
How Common is Spotting During Birth Control Use?
How often spotting happens depends on the method and timing. Up to half of new combined oral contraceptive users report some breakthrough bleeding in the first three months, while progestin-only methods and implants can cause irregular bleeding for a longer period. Factors that increase spotting include ultra‑low‑dose estrogen pills, missed or late pills, smoking, and medicines that change hormone metabolism. Most breakthrough bleeding decreases as the lining stabilizes; many people see improvement by three to six months, although progestin-only users may experience more persistent irregularity. Knowing these prevalence ranges can help you decide when to monitor and when to seek a method change or medical evaluation.
What Are the Common Causes of Spotting on Contraception?
Spotting while on contraception can stem from several causes: hormonal adjustment, inconsistent dosing, drug interactions that lower hormone levels, or unrelated medical issues. Identifying the cause directs the right response. Progestin tends to thin the endometrium, making it prone to small breaks; missed or late pills create abrupt hormone dips that trigger bleeding; and conditions such as pregnancy, STIs, polyps, or fibroids can also cause irregular bleeding. Below are the most frequent causes and a quick table that links cause, mechanism, and expected timeline to help set realistic expectations.
Common causes include:
Hormonal adjustment after starting or switching contraception.
Missed, late, or interacting medications that reduce hormone levels.
Pregnancy-related bleeding (including implantation) and infections.
Structural issues such as fibroids or polyps that cause irregular bleeding.
The following table summarizes cause, mechanism, and expected timeline so you can match symptoms to likely explanations and next steps.
Different causes produce spotting through specific biological mechanisms and tend to follow predictable timelines.
Cause
Mechanism
Typical Timeline
Hormonal adjustment (start/switch)
Endometrial instability from progestin or low estrogen
Days–months; often improves within 3–6 months
Missed or late pills / drug interactions
Acute drop in circulating hormones causing breakthrough bleeding
Immediate to 1–2 cycles; consider a pregnancy test if several pills were missed
Pregnancy or implantation bleeding
Early placental changes can cause light bleeding
Early pregnancy timing; evaluate promptly if suspected
Infection (STI)
Local inflammation and a fragile cervix lead to irregular spotting
Days–weeks; treatable with appropriate therapy
Fibroids or polyps
Local structural bleeding from lesions
Ongoing until lesion is treated or removed
How Do Hormonal Adjustments Lead to Spotting?
Hormonal adjustments cause spotting because progestin-rich states thin the endometrium, creating a fragile surface that can bleed with small hormonal shifts or minor irritation. When estrogen is low or fluctuates, tiny blood vessels in the superficial lining may break and produce light bleeding rather than a coordinated menstrual withdrawal. This is common with ultra‑low‑dose combined pills or after switching to progestin-only methods; the lining needs time to remodel to the new hormone environment. For most people, reassurance and watchful waiting for about three months is reasonable unless bleeding is heavy or accompanied by worrying symptoms — in which case further evaluation is needed. This mechanism also explains why short-term estrogen supplementation under provider supervision sometimes helps selected patients.
Can Missed or Late Pills Cause Breakthrough Bleeding?
Yes. Missing or taking pills late disrupts the steady hormone levels that keep the lining stable. Sudden drops in hormones often trigger spotting or heavier breakthrough bleeding. What to do right away depends on the pill type and timing, but common guidance is to take the most recent missed pill as soon as you remember and use backup protection if multiple pills were missed. If you had unprotected sex during the lapse, a pregnancy test may be appropriate. Occasional light spotting after a single missed pill doesn’t always mean contraceptive failure, but repeated lapses raise both bleeding irregularity and pregnancy risk. Consistent daily dosing and checking for drug interactions are important preventive steps.
How Does Spotting Vary by Types of Birth Control?
Bleeding patterns vary because each delivery method and hormone mix affects the endometrium and systemic levels differently. Progestin-only methods (pills, implants, hormonal IUDs, injectables) commonly cause more unpredictable spotting because they create a chronically thin, fragile lining. Combined estrogen–progestin methods usually cause spotting mainly during the initial adjustment period. The copper IUD, being non-hormonal, typically increases menstrual bleeding rather than causing isolated spotting. The table below compares typical spotting patterns and helpful notes for common methods.
The following table compares methods so you can anticipate likely experiences and discuss options with your provider.
Method
Typical Spotting Pattern
Prevalence / Notes
Combined oral contraceptives (COC)
Early-cycle spotting that usually settles within ~3 months
Common — up to about 50% of new users with low-dose pills
Progestin-only pill (POP)
Irregular, often unpredictable spotting
Greater long-term irregularity compared with COC
Hormonal IUD
Irregular spotting initially; periods often lighter over time
Spotting common first 3–6 months; bleeding often reduces later
Copper IUD
Generally heavier menstrual bleeding, less isolated spotting
May increase flow and cramping
Implant
Frequent irregular spotting early and sometimes long-term
High early irregular bleeding; many improve over months
Depo-Provera shot
Irregular bleeding or prolonged spotting; some develop amenorrhea
Patterns vary; irregularity common in initial months
What Spotting Patterns Are Associated with Oral Contraceptives?
Combined pills commonly cause breakthrough spotting early as the body adjusts to exogenous estrogen and progestin. Many users see improvement within three cycles as the lining stabilizes. Low‑dose or ultra‑low‑dose estrogen pills are more likely to cause early spotting because the estrogen may not be enough to stabilize the lining right away. Progestin‑only pills often cause more persistent, unpredictable bleeding that can last beyond six months for some people. Knowing these patterns helps decide whether to wait a few cycles or consider an earlier change.
How Do IUDs, Implants, and Other Devices Affect Spotting?
Hormonal devices like levonorgestrel IUDs and implants often cause irregular spotting in the first months because of local progestin effects on the lining; many people using an IUD later report lighter periods or no periods at all, while implants may continue to produce irregular bleeding longer. The copper IUD usually increases overall menstrual bleeding and cramping rather than causing isolated spotting — an important distinction when choosing between hormonal and non‑hormonal options. Injectable contraceptives also change bleeding patterns: some users have irregular or prolonged bleeding, others develop amenorrhea with continued use. These device-specific expectations help guide counseling and decisions about continuing or changing methods.
When Should You Worry About Spotting on Birth Control? Signs to Seek Medical Advice
Most spotting is harmless, but certain signs call for prompt clinical assessment because they suggest infection, significant blood loss, or other problems. Red flags include heavy bleeding that soaks a pad or tampon every hour, severe pelvic pain, fever, persistent bleeding lasting longer than one to two weeks, bleeding after sex, or pregnancy symptoms such as a missed period and nausea. The short triage checklist and table below connect symptoms to urgency and suggested actions so you can decide whether to seek urgent care, schedule a routine appointment, or monitor at home. If you’re unsure, contacting a clinician for personalized advice is appropriate.
Key red-flag symptoms to watch for include:
Heavy bleeding or passing large clots, or rapid saturation of protection.
Severe pelvic or abdominal pain, dizziness, or fainting sensations.
Fever, foul-smelling discharge, or other signs of infection.
Bleeding that continues beyond about two weeks or bleeding after sex.
These signals help distinguish harmless adjustment bleeding from conditions that need immediate attention. The next table pairs symptoms with recommended actions.
Symptom
Why it's Concerning
Suggested Action
Heavy bleeding (soaking pad/hour or large clots)
Risk of significant blood loss and anemia
Seek urgent care or ER evaluation
Severe pelvic pain or fainting
Possible torsion, infection, or ectopic pregnancy
Urgent evaluation and imaging as needed
Fever, foul discharge
Suggests pelvic infection or PID
Contact provider promptly for testing and treatment
Bleeding >2 weeks or postcoital bleeding
May indicate structural lesions like polyps or other disease
Schedule evaluation within 1–2 weeks; consider ultrasound
What Are Red Flag Symptoms Like Heavy Bleeding or Severe Pain?
Heavy bleeding — defined as saturating a pad or tampon in an hour or passing large clots — can lead to anemia or hemodynamic instability if it continues and should prompt emergency care. Severe pain that disrupts daily life or comes with faintness or low blood pressure is another urgent warning sign; it could mean ectopic pregnancy, ovarian torsion, or a serious infection. Fever and foul-smelling discharge point to pelvic inflammatory disease or another infection that needs antibiotics and evaluation. Recognizing these signs and acting quickly reduces risk and speeds diagnosis and treatment.
When is It Important to Consult a Healthcare Provider?
Contact your healthcare provider promptly if spotting is paired with any red-flag signs, if bleeding lasts longer than about two weeks, or if you suspect pregnancy despite contraception. During an evaluation, clinicians typically do a pregnancy test, STI screening, pelvic exam, and pelvic ultrasound when indicated to look for causes such as retained tissue, structural lesions, or ectopic pregnancy. For persistent but non‑urgent spotting, schedule a routine appointment within one to two weeks so problems can be investigated without an unnecessary ER visit. Preparing a concise symptom log — dates, bleeding description, related symptoms, and contraceptive details — helps clinicians triage faster and more accurately.
Right after listing when to consult, it helps to know what supportive options exist for triage and care navigation.
Her Smart Choice can assist with triage and connect you to appropriate clinical care when spotting raises concern, offering non‑promotional guidance to help decide whether you need urgent care or routine evaluation.
How to Stop Spotting on Birth Control: Effective Management and Prevention Tips
Reducing or stopping spotting starts with consistent, correct use of your method and addressing modifiable factors like smoking or interacting medications. Providers may suggest short‑term measures such as NSAIDs for cramping, temporary estrogen supplementation for select combined‑pill users, or changing to a different formulation or method if bleeding persists and affects quality of life. Medication reviews, lifestyle adjustments, and clear guidance on missed‑dose management are practical first steps that help people minimize irregular bleeding. Below are concrete actions and common medical options used to manage persistent spotting.
Practical actions to reduce spotting include:
Stick to a strict dosing schedule for pills — set daily reminders to avoid missed doses.
Review all prescription, over‑the‑counter medicines, and supplements with a clinician to spot interactions.
Consider smoking cessation and healthy weight management as part of long‑term stabilization.
What Lifestyle Changes Can Reduce Spotting?
Smoking speeds the breakdown of some hormones and is linked to more breakthrough bleeding, so quitting often improves bleeding patterns and has wide health benefits. Stabilizing weight and eating a balanced diet can support steady hormone balance for some people. Reviewing OTC and prescription medicines — especially enzyme‑inducing drugs — with a clinician can identify interactions that lower contraceptive hormone levels and trigger spotting. Pairing these lifestyle steps with consistent contraceptive use supports long‑term stability and may reduce the need for medical changes.
What Medical Treatments or Adjustments Help Manage Spotting?
If lifestyle measures aren’t enough, clinicians might recommend short‑term estrogen supplementation, a temporary course of combined pills, or switching to a formulation with more estrogen to stabilize the lining for combined‑method users. For progestin‑only users, options include trying a different progestin formulation, switching to a combined method if appropriate, or treating any underlying condition found on evaluation. NSAIDs can reduce bleeding‑related prostaglandins and relieve cramping; surgical or procedural options address structural causes like polyps or fibroids. Any medication or method change should be supervised by a healthcare provider to keep contraception safe and effective. What are the types of birth control methods?
How Can Her Smart Choice Support You with Spotting on Birth Control?
Her Smart Choice provides supportive, evidence‑informed reproductive health guidance focused on education, triage, and care navigation — not on prescribing treatment directly. We help users interpret spotting patterns and connect them to appropriate care. Services include clear educational resources about common bleeding patterns, clinician consultations for personalized assessment and contraceptive counseling, and referrals or care navigation to local providers for in‑person testing or procedures. Our role is to reassure, clarify options, and help prioritize urgency so people get timely evaluation when needed. If you’re unsure whether your spotting needs immediate attention, Her Smart Choice can help you organize your symptom history, identify red flags, and suggest the best next step.
What Services and Guidance Does Her Smart Choice Provide?
Her Smart Choice offers a range of supportive services: educational materials about contraception and bleeding patterns, structured triage conversations to assess urgency, and clinician-led consultations for personalized counseling. We also help with care navigation and referrals when diagnostic testing, imaging, or in‑person treatment is required, connecting you to appropriate clinical resources while emphasizing patient-centered, evidence‑based decision-making. These services are designed to supplement clinical care by improving understanding and helping people prepare for effective medical evaluations. For many users, this supportive pathway reduces anxiety and speeds access to the right level of care.
How to Access Personalized Reproductive Health Support?
To get the most from a consultation, prepare a brief symptom log with dates of spotting, a description of bleeding and any clots, your contraceptive method and how you’ve been using it, and any symptoms such as pain or fever. In a triage or consultation session, expect a focused review of your history, a discussion of likely causes, and clear recommendations — whether that’s urgent evaluation, routine follow‑up, or conservative management. Her Smart Choice helps by outlining what clinicians will want and by recommending next steps, whether that means watching for a few cycles, scheduling tests, or arranging referrals. Documenting your experiences and questions ahead of time makes visits more efficient and increases the chance of a timely, accurate assessment.
Prepare: Track bleeding dates, contraceptive details, and symptoms.
Consult: Use our educational resources or schedule a triage conversation to clarify urgency.
Navigate: If needed, request a referral or guidance for local clinical evaluation.
These steps help move you from uncertainty to a clear plan so spotting can be evaluated appropriately and efficiently.
Frequently Asked Questions
What should I do if I experience spotting after switching birth control methods?
Spotting after switching methods is often a normal adjustment as your body adapts to new hormones. If it continues beyond three to six months or comes with other concerning symptoms, check in with your healthcare provider. They can determine if the bleeding is a benign response or if a method change is warranted. Keeping a simple record of dates and symptoms helps your provider give the best advice.
Can stress affect spotting while on birth control?
Yes. Stress can change your hormone balance and affect your cycle, which may lead to spotting while on birth control. If you notice more breakthrough bleeding during stressful times, consider stress‑management techniques like mindfulness, regular exercise, or counseling. If spotting persists or gets worse, consult your healthcare provider for evaluation and support.
Is there a difference in spotting patterns between hormonal and non-hormonal birth control?
Yes. Hormonal methods (pills, patches, rings, hormonal IUDs, implants, shots) commonly cause irregular spotting as the body adjusts. Non‑hormonal methods, like the copper IUD, more often lead to heavier menstrual bleeding rather than isolated spotting. Knowing these differences can help you set realistic expectations for whichever method you choose.
How can I differentiate between spotting and a potential pregnancy issue?
Spotting is usually light, brown or pink, and doesn’t require protection; pregnancy‑related bleeding can have other signs such as cramping, nausea, or a missed period. If you suspect pregnancy or experience heavy bleeding, severe pain, or other concerning symptoms, take a pregnancy test and contact your healthcare provider for further evaluation.
What lifestyle factors can exacerbate spotting on birth control?
Factors that can make spotting more likely include smoking, excessive alcohol use, significant weight changes, and certain medications that interfere with hormone levels. Smoking is a key contributor because it speeds hormone metabolism. Healthy lifestyle choices — quitting smoking, balanced diet, and regular activity — can help stabilize hormones and may reduce spotting.
Are there any over-the-counter treatments for managing spotting?
Over‑the‑counter NSAIDs (like ibuprofen) can help with cramping and may reduce bleeding by lowering prostaglandin activity. However, check with a healthcare provider before starting any medication to make sure it’s appropriate and won’t interfere with your method. Always follow dosing instructions on the label or your provider’s advice.
How can I prepare for a consultation regarding spotting on birth control?
Before your appointment, keep a symptom log with dates of spotting, the amount and color of bleeding, any clots, and related symptoms (pain, fever). Note your contraceptive method, how consistently you use it, and any other medicines or supplements you take. This information helps your provider understand the pattern quickly and recommend the right next steps.
Conclusion
Understanding spotting on birth control — why it happens and how it’s managed — can help you feel more confident about your reproductive health. Recognizing that breakthrough bleeding is often normal, and knowing the signs that need medical attention, helps you keep contraception effective and gives you peace of mind. For personalized support and care navigation, consider reaching out to Her Smart Choice — we can help you interpret what’s happening and connect you with the right care. Take the next step in your reproductive health with clear information and a plan.
This guide helps you understand exactly when oral contraceptives begin protecting against pregnancy and gives clear, actionable steps so you can use them with confidence. You’ll get straightforward timelines for combined oral contraceptives (COCs) and progestin-only pills (POPs or “mini‑pills”), learn the biological reasons the timelines differ, and find precise rules for common start methods (Day 1, Quick Start, Sunday Start). The article also walks through missed‑pill actions, when to use backup contraception, and special situations such as postpartum use or starting after an abortion. The practical takeaways are simple: types of birth control methods usually give immediate protection; non‑Day 1 COCs generally need about 7 days of backup; non‑Day 1 POPs generally need about 48 hours.
How Long Does It Take for Birth Control Pills to Start Working?
Here’s a concise summary of when pills become effective and why that timing matters. Combined pills mainly prevent pregnancy by stopping ovulation and changing cervical mucus so sperm can’t reach an egg. Progestin‑only pills mostly thicken cervical mucus and sometimes suppress ovulation, which makes precise timing and daily consistency more important. Practically speaking, starting a combined pill on Day 1 of your period usually gives protection right away because ovulation for that cycle is already unlikely. If you start a combined pill at another point, you’ll usually need a short waiting period while ovulation suppression kicks in. For most POPs, a Day 1 start also gives immediate coverage, but starting at other times commonly requires about 48 hours of backup while mucus changes take effect. Knowing how each method works will help you pick the right start and use backup correctly when needed.
This article exists to explain when pills start working and to give clear, evidence‑informed steps so you can manage contraception confidently.
Different start scenarios change how quickly protection begins. The table below gives quick rules and backup recommendations so you can see the most common situations at a glance.
Pill Type / Start Scenario
Start Method
Time to Effective Protection
Backup Needed (Yes/No & Duration)
Combined pill — Day 1 start
Day 1 of period
Immediate protection (same cycle)
No backup needed if correctly started on Day 1
Combined pill — Quick/Sunday start
Quick Start or Sunday Start
Protection after about 7 days
Yes — use backup for 7 days
Progestin-only pill — Day 1 start
Day 1 of period
Immediate protection
No backup needed if correctly started on Day 1
Progestin-only pill — Other start
Quick Start or other
Protection after ~48 hours (2 days)
Yes — use backup for 2 days
The short rules to remember: Day 1 starts give immediate coverage; combined pills started at other times generally need about seven days; progestin‑only pills started at other times generally need about two days. The next section explains each start method in more detail to help you choose the right approach for your situation.
When Is the Combined Birth Control Pill Effective After Starting?
Combined oral contraceptives prevent pregnancy mainly by stopping ovulation and by changing cervical mucus. If you start a combined pill on the first day of your period (Day 1), most guidance treats you as protected immediately because the hormones align with that cycle’s natural timing. If you begin a combined pill at another point in your cycle (Quick Start or Sunday Start), it typically takes roughly seven days for ovulation suppression and mucus changes to fully reduce pregnancy risk, so use backup during that time. Keep in mind that vomiting, severe diarrhea, or medications that interact with the pill can lower absorption and may extend the time you need backup — in those cases check with your clinician or follow the manufacturer’s instructions.
How Quickly Does the Mini Pill Become Effective?
Progestin‑only pills (POPs) work mainly by thickening cervical mucus and depend heavily on strict daily timing. When taken on Day 1 of bleeding, most POPs provide immediate protection for that cycle because ovulation is unlikely and mucus changes set in quickly. If you start a POP on another day, plan to use backup contraception for about 48 hours while the mucus response becomes reliable. POP effectiveness also depends on taking the pill at the same time every day — some formulations have a narrow window (often around three hours); doses taken outside that window may count as missed and require immediate backup. The next section breaks down start methods and backup requirements step by step.
Progestin-Only Pills (POPs): Safety, Efficacy, and Adherence Considerations Progestin‑only pills are commonly recommended for people who can’t take estrogen (for example, while breastfeeding or with certain health conditions). They have a wide safety profile and are effective when taken correctly, which is why some experts have supported wider access without a prescription. Because POPs rely on precise daily dosing, users need clear guidance about missed or delayed pills; unlike for combined pills, we have less data showing brief nonadherence is harmless with low‑dose POPs. Source: protocol and research summaries on POP adherence and effectiveness (M. Creinin et al., 2021).
What Are the Different Start Methods for Birth Control Pills and Their Effectiveness?
The start method you choose affects how quickly you’re protected and how convenient the schedule is. The three common approaches are Day 1 start, Quick Start, and Sunday Start. Day 1 starts usually give immediate protection for both combined pills and POPs because they coincide with the natural menstrual cycle. Quick Start lets you begin right away on the day you get the pills, which avoids waiting for your next period but generally requires short‑term backup (7 days for combined pills, 2 days for POPs). Sunday Start is chosen for convenience so reminders fall on a consistent weekday; its backup rules match Quick Start and depend on pill type. The table below summarizes procedures, benefits, and when backup is needed.
Start Method
Typical Procedure
Pros
When Backup Is Required
Day 1 start
Begin on the first day of menstrual bleeding
Immediate protection for most pill types; straightforward rules
Generally not required if correctly started on Day 1
Quick Start
Begin immediately on the day you receive the pill
Fast initiation; avoids waiting
COC: 7 days; POP: 2 days
Sunday Start
Begin on the first Sunday after your period begins or when prescribed
Matches weekly routine for easier reminders
COC: 7 days; POP: 2 days
Choosing the right start method depends on how quickly you need protection and what fits your routine. The following section lists the main reasons to use backup contraception and exactly how long to use it, so you can act with confidence if circumstances change.
How Does Starting on Day 1 of Your Period Affect Effectiveness?
Starting on Day 1 lines up the pill’s hormones with your cycle, lowering the chance of ovulation that cycle and typically giving immediate contraceptive protection. Since ovulation usually happens mid‑cycle, beginning on the first day of bleeding prevents the later steps required for pregnancy in that cycle. Exceptions include the postpartum period, breastfeeding, or when you’re taking interacting medications — in those situations a clinician may recommend different timing or temporary backup. For most people, Day 1 is the simplest way to avoid a waiting period and begin protection right away.
What Is the Quick Start and Sunday Start Method, and When Is Backup Needed?
Quick Start means you start the pill the day you get it instead of waiting for your period; Sunday Start means you begin on the first Sunday after your chosen start date. Both are convenient and can improve adherence, but they usually require short‑term backup because protection takes a few days to build. For combined pills, use condoms or avoid sex for seven days after starting with Quick or Sunday Start; for progestin‑only pills, use backup for two days. If you’ve had recent unprotected sex or suspect pregnancy, consider testing or clinical advice before Quick Start. These start options let you begin on your schedule while staying protected with the recommended backup rules.
When and Why Do You Need Backup Contraception with Birth Control Pills?
Use backup contraception whenever your pill protection is uncertain or temporarily interrupted — for example, after non‑Day 1 starts, missed or late pills, drug interactions, or vomiting/diarrhea. Pills rely on steady hormones and mucus changes; anything that disrupts hormone levels or timing can create a window when pregnancy is possible. A simple rule of thumb helps decision‑making: for combined pills use backup for seven days after a late start or multiple missed pills; for progestin‑only pills use backup for 48 hours in comparable situations. Backup options include condoms or abstinence; emergency contraception is a separate option if you had unprotected sex during a high‑risk window. The lists below show common scenarios that require backup and what to do right away.
Common situations that require backup contraception:Starting pills not on Day 1 (Quick/Sunday starts) Missing one or more pills or taking pills late beyond the allowed window Vomiting or severe diarrhea within a few hours of taking a pill Taking medications that interact and reduce contraceptive effectiveness
Immediate actions to take when backup is needed:Use condoms or avoid sex until the backup period ends Keep taking your pills as directed (don’t skip more doses) Consider emergency contraception if you had recent unprotected sex Contact a clinician if you missed multiple pills or are on interacting medications
How Long Should Backup Contraception Be Used for Combined Pills?
For combined oral contraceptives, the standard waiting period after a non‑Day 1 start or after missed pills is seven days. This gives the hormones time to reliably suppress ovulation and establish protective mucus changes. If you miss a single combined pill but take it within about 24 hours, you’ll usually maintain protection; missing multiple pills or having longer gaps typically triggers the seven‑day backup rule and may prompt consideration of emergency contraception if you had unprotected sex. Helpful prevention tips include setting daily reminders, using a pill organizer, and using condoms during the seven‑day backup window. If vomiting, interactions, or many missed doses occur, check with your clinician.
How Long Is Backup Needed for the Mini Pill?
For progestin‑only pills, backup is usually required for 48 hours (two days) after a non‑Day 1 start or after a missed or late dose that falls outside the pill’s allowed timing window. POPs rely on consistent hormone levels and mucus thickness, so even brief delays can reduce effectiveness — hence the shorter but strict backup interval. If you miss a POP dose beyond its allowed window, take the missed pill as soon as you remember and use condoms or avoid sex for 48 hours. Simple strategies like phone alarms, carrying extra packs, and tying pill time to a daily habit help avoid lapses that would trigger the backup rule.
What Should You Do If You Miss a Birth Control Pill?
Knowing pill‑type specific steps helps reduce pregnancy risk and tells you when to use backup or seek emergency contraception. The main difference is between combined pills and progestin‑only pills: combined pills often have a longer grace period for one missed dose and different advice for multiple misses; POPs have a very narrow timing window, so many late doses count as missed. Immediate steps include taking the missed pill as soon as you remember, continuing the pack, and starting backup if you’re outside the acceptable window. The table below summarizes common scenarios and the recommended actions so you can act quickly.
Pill Type
Miss Window
Immediate Steps
Backup / Emergency Contraception Recommendation
Combined (1 missed)
Missed 1 active pill (<24 hours usually)
Take the missed pill ASAP, then continue the pack
Generally no backup if taken within the window; otherwise use backup for 7 days
Combined (≥2 missed)
Two or more active missed pills
Take the most recent missed pill immediately, discard others if instructed, continue the pack
Use backup for 7 days; consider emergency contraception if you had unprotected sex
Progestin-only (missed timing)
Dose taken outside allowed time window (e.g., >3 hours)
Take the missed pill ASAP, then resume your regular schedule
Use backup for 48 hours; consider emergency contraception if you had unprotected sex
These steps will help you restore protection quickly. The next sections give simple, stepwise instructions for each pill type so you can follow the right actions under stress.
How to Manage Missed Combined Pills to Maintain Protection?
If you miss a single combined pill and can take it within about 24 hours, take it as soon as you remember and keep taking the rest of the pack — most guidance treats this as maintaining protection. If you miss two or more active combined pills, take the most recent missed pill immediately (discard earlier missed pills if directed), continue the pack, and use backup contraception for seven days. If you had unprotected sex in the days before missing pills, emergency contraception may be appropriate — contact a clinician to discuss timing and options. After an episode of missed pills, consider stronger adherence supports like daily alarms, pill boxes, or apps to help avoid future gaps.
What Are the Guidelines for Missed Mini Pills and Timing Windows?
For progestin‑only pills, a missed dose usually means taking the pill outside the strict daily timing window (commonly about three hours for many POPs). That missed timing can immediately reduce protection. If you miss or take a POP late, take the missed pill as soon as you remember and then use backup contraception for 48 hours while keeping to your daily schedule. If you had unprotected intercourse during the missed window, consider emergency contraception and contact a clinician promptly. Practical prevention strategies — setting a fixed daily time, alarms, and carrying pills when you travel — are very effective at avoiding missed‑dose problems.
How Do Special Situations Affect When Birth Control Pills Start Working?
Certain situations — childbirth and breastfeeding, recent abortion or miscarriage, or switching between pill types — can change recommended start timing and backup needs. After delivery, especially while breastfeeding, clinicians often avoid estrogen‑containing pills at first because estrogen can reduce milk supply; progestin‑only pills or non‑hormonal methods may be preferred early on, and protection timing will follow the specific method’s rules. After abortion or miscarriage, many protocols allow immediate pill start to provide prompt protection, though backup needs depend on timing and method. When switching pills, keep continuity (finish a pack or follow your clinician’s instructions) to avoid gaps; backup might be necessary during the transition. The table below outlines typical rules for these scenarios so you know what to expect.
Scenario
Typical Rule
Backup Needed
Postpartum (non-breastfeeding)
May start combined pills after a short interval
Often follows Day 1 or Quick Start rules; backup may be required
Breastfeeding
Estrogen-containing pills are often delayed; POPs are preferred
Backup rules depend on timing and clinician advice
After abortion/miscarriage
Immediate start is often permitted
Backup may not be needed in some cases; follow clinician guidance
These scenario‑based rules show why personalized clinical advice matters in special circumstances. The following subsections give practical guidance for postpartum and post‑abortion situations.
When Does Birth Control Become Effective After Childbirth or While Breastfeeding?
Timing after childbirth depends on breastfeeding and your medical history. Because estrogen can reduce milk supply for some people, clinicians often delay estrogen‑containing combined pills while breastfeeding and prefer progestin‑only options early on. If a POP is started immediately after delivery, the usual POP timing rules apply and backup depends on whether it was a Day 1 start. If you are not breastfeeding, combined pills may be started according to local guidance, with Day 1 or Quick Start rules and the usual backup requirements. Because personal health factors and breastfeeding goals affect the best choice, check with your clinician for individualized advice before starting or changing pills after childbirth.
How Does Starting Birth Control After Abortion or Miscarriage Impact Effectiveness?
After an abortion or miscarriage, many protocols allow immediate initiation of oral contraceptives because the uterus is not pregnant and rapid protection is often useful. Whether you need backup depends on the exact timing and the method used: starting on Day 1 of bleeding often gives immediate protection in guidance from some providers, while Quick Start generally requires the standard 7‑day (COC) or 2‑day (POP) backup. Immediate initiation can help prevent another unintended pregnancy and simplify follow‑up care, but confirm there are no contraindications and arrange appropriate follow up. If you’re unsure or had recent unprotected sex, consider pregnancy testing and talk to a clinician about emergency contraception options.
What Are Common Myths and FAQs About Birth Control Pill Effectiveness?
Several myths about pill effectiveness persist. Clear, direct answers help reduce confusion and support correct use. Two frequent concerns are whether pregnancy is possible during the first week after starting pills and whether pills work immediately after you begin. The short answers are: yes, pregnancy is possible in the first week if you didn’t start on Day 1 and didn’t use backup; and no, pills are not always effective immediately unless started on Day 1 — non‑Day 1 COCs generally need seven days and POPs generally need two days of backup. Below are quick myth‑busting points and a small FAQ that cover the most practical questions people ask.
Can you get pregnant during the first week of birth control? Yes — if you did not start on Day 1 and did not use backup, the first week can carry risk, especially with Quick or Sunday Starts.
Does missing one pill always cause pregnancy? No — a single missed combined pill taken within the allowed window usually preserves most protection, but multiple missed pills increase risk and typically require backup.
Do stomach bugs make pills ineffective? Vomiting or severe diarrhea within a few hours of taking a pill can reduce absorption; treat the dose as missed and follow backup guidance.
Can other medicines stop my pill from working? Some medicines and supplements interact with hormonal contraception and can reduce effectiveness; check with a clinician or pharmacist when starting new drugs.
These quick answers address common concerns; the final subsections give concise responses to two widely searched questions to support clarity and practical decision making.
Can You Get Pregnant During the First Week of Birth Control?
Yes — pregnancy is possible during the first week if you didn’t start on Day 1 and didn’t use backup during a Quick or Sunday Start. The actual risk depends on where you are in your cycle and whether you had recent unprotected sex, because ovulation can occur before the pill’s full protective effects are established. If you began with a non‑Day 1 start and had unprotected intercourse, consider emergency contraception depending on timing, and use backup contraception for the recommended seven days for COCs or two days for POPs.
Does Birth Control Work Immediately After Starting?
Birth control pills work immediately only when started on Day 1 of bleeding for most protocols. Otherwise, you must wait the standard protection window — about seven days for combined pills and about two days for progestin‑only pills. The Day 1 rule applies because it aligns with the natural cycle and lowers the chance of ovulation that cycle. With Quick Start or Sunday Start, use backup for the specified period until hormonal and mucus‑based protection is established.
Frequently Asked Questions
What should I do if I miss multiple birth control pills?
If you miss two or more active combined pills, take the most recent missed pill as soon as you remember and discard any earlier missed pills if directed. Continue taking the rest of the pack on schedule, but use backup contraception for the next seven days. If you had unprotected sex in the days before the missed pills, talk with a healthcare provider about emergency contraception options.
Can I switch between different types of birth control pills?
Yes — you can switch pill types, but do it in a way that avoids gaps in protection. Follow your clinician’s instructions or the manufacturer’s guidance: either finish your current pack or begin the new pill as recommended. Backup contraception may be needed during the transition if there’s any gap. When in doubt, consult your healthcare provider for personalized advice.
How do antibiotics affect birth control pill effectiveness?
Most common antibiotics do not reduce pill effectiveness, but there are exceptions — rifampin and similar medications can interfere with hormonal contraception. If you’re prescribed antibiotics that may affect the pill, use backup contraception during treatment and for at least seven days after finishing, or follow your provider’s guidance. Always check with your clinician or pharmacist about specific interactions.
What are the signs that my birth control pill is not working?
Possible signs include unexpected bleeding or spotting, missed periods, or symptoms of pregnancy such as nausea or breast tenderness. If you notice these signs, especially after unprotected sex, take a pregnancy test and contact your healthcare provider. Also review your pill‑taking routine to make sure you’re taking pills on schedule.
Is it safe to take birth control pills continuously without a break?
Many people safely use pills continuously to skip periods or reduce symptoms, and some formulations are designed for continuous use. Continuous use may be recommended for specific medical reasons, but it’s best to discuss this with your provider to confirm it’s appropriate for you and to choose the right regimen.
What should I do if I experience side effects from birth control pills?
If you have side effects such as nausea, headaches, or mood changes, talk with your healthcare provider. They can help determine whether side effects are likely to settle or whether switching to a different formulation or method would be a better option. Don’t stop taking your pills without medical advice unless directed to do so.
Conclusion
Knowing when birth control pills start protecting you makes it easier to use them correctly and confidently. Remember the simple timelines: Day 1 starts usually give immediate protection; combined pills started at other times typically need about seven days of backup; and progestin‑only pills started at other times typically need about 48 hours. Choosing the right start method, sticking to a daily routine, and using backup when needed will keep you protected. If you have special circumstances or are unsure, check with your healthcare provider for personalized guidance and explore our resources for more tips on managing your contraception.
An abortion - whether medication-based or surgical - sets off a series of physical and emotional changes as your body settles back toward its pre-pregnancy state. This guide walks through common physical symptoms (bleeding, cramping, discharge, breast changes), the hormonal shifts involved (hCG, estrogen, progesterone), and typical emotional responses so you know what’s normal and when to get care. People often want clear timelines, practical self-care steps, and reassurance about fertility and future family planning; this article delivers those answers in plain, evidence-informed language. You’ll find a recovery timeline, symptom-by-symptom explanations, pain and bleeding management tips, warning signs to watch for, and contraception planning. Each section includes actionable checklists and simple comparisons to help you follow your recovery during the hours, days, and weeks after the procedure. Read on to learn common recovery patterns, how hormones affect what you feel, and where to find support if you need it.
How long does the abortion recovery timeline last?
“Recovery” refers to the time your body takes to expel pregnancy tissue, shrink the uterus back to its usual size, and for hormone levels and symptoms like bleeding and cramping to settle. How long that takes depends on the type of procedure (medical versus surgical), how far along the pregnancy was, and individual health differences. For some people, the most intense symptoms last a few hours or days; for others, light spotting or intermittent symptoms continue for several weeks. Early milestones commonly include heavier bleeding and stronger cramping in the first 4–6 hours (and sometimes up to 24–72 hours), with a gradual taper in bleeding and pain over the next 1–2 weeks for many people. Knowing these stages can help you plan rest, work, and follow-up care — and reduce worry about what’s normal.
Quick snapshot: the table below summarizes typical symptom durations for medical versus surgical abortion so you can compare what to expect in the early recovery phase.
Symptom
Typical Duration (Medical Abortion)
Typical Duration (Surgical Abortion)
Heavy bleeding/cramping (intense)
4–24 hours, up to 72 hours in some
12–48 hours
Ongoing lighter bleeding/spotting
Up to 2–4 weeks
1–2 weeks
Severe cramping requiring stronger pain relief
First 1–3 days
First 24–48 hours
When to expect follow-up confirmation
1–2 weeks (may require hCG or clinic confirmation)
Often within 1–2 weeks or at clinician’s schedule
This comparison shows that medical abortions often involve longer spotting as medication causes the body to pass tissue over time, while surgical procedures usually lead to a shorter, more immediate recovery period. If you’d like personalized follow-up or extra reassurance about your recovery, Her Smart Choice offers compassionate information and support tailored to post-abortion needs to help you decide on clinical follow-up or self-care steps.
What is the typical duration of physical recovery after abortion?
Physical recovery generally follows a familiar pattern: the first hours and days are the most intense, then symptoms ease over days and weeks as hormones and uterine size return toward baseline. Most people have the heaviest bleeding and strongest cramping within the first 4–24 hours, with noticeable improvement by the end of week one. Light bleeding or spotting may continue intermittently for up to 2–4 weeks for many. Systemic symptoms such as tiredness or mild nausea usually resolve within a few days. Knowing this typical arc helps you plan pain control, rest, and a safe return to daily activities while recognizing when to seek medical help.
How does recovery differ between medical and surgical abortions?
Medical abortion uses medication to trigger uterine contractions and tissue passage, so bleeding and cramping can be intense but often occur over several hours to days, with spotting that may continue for a few weeks. Surgical abortion usually produces a shorter recovery: bleeding and cramps are often worst immediately after the procedure and then decline more quickly over the next days. Follow-up also differs: medical abortion may need a clinic visit or hCG check to confirm completion, while surgical abortion often includes immediate clinical confirmation. These differences influence choices about pain control, timing for returning to work, and scheduling contraception or follow-up visits.
What are the common physical changes after an abortion?
Many physical signs after an abortion are expected and reflect the body’s hormonal and physical adjustments as pregnancy tissue resolves and the uterus contracts back to its usual size. Typical changes include bleeding that can range from heavy flow to light spotting, uterine cramping, vaginal discharge as tissues heal, and breast tenderness as pregnancy hormones fall. You may also feel tired, slightly nauseated, dizzy, or notice temporary changes in appetite or sleep — these usually improve over days to a few weeks. Additional insights can be found in hormonal shifts after abortion.
Below is a practical chart linking common symptoms with likely causes and simple self-care steps to manage each during recovery.
Symptom
Cause / Mechanism
Suggested Self-Care
Bleeding (heavy to spotting)
Uterine shedding of pregnancy tissue and hormonal withdrawal
Use pads, rest during heavy flow, avoid tampons for advised period, monitor volume
Cramping
Uterine contractions to expel tissue and shrink the uterus
OTC pain relief, heat packs, paced rest, light movement as tolerated
Vaginal discharge
Healing of cervix and endometrial shedding
Maintain hygiene, avoid baths or douching for advised period, watch for foul odor
Breast tenderness
Sudden drop in pregnancy hormones (estrogen/progesterone)
This table explains why symptoms occur and simple home steps that often help. If you notice unusual signs like a foul odor, fever, or rapidly worsening pain, contact a clinician promptly.
What post-abortion symptoms should you expect?
You can expect a variety of symptoms that differ in intensity between people; the most common are bleeding, cramping, breast tenderness, and short-term systemic effects such as fatigue. Bleeding may be heavy with clots the first day or two, then taper to light spotting over weeks. Cramping is often like menstrual cramps but can be stronger at first. Breast tenderness comes from the sudden hormone drop and usually eases over days to a few weeks. Tracking timing and intensity helps you tell normal recovery from signs that need medical attention.
How do hormonal shifts affect your body after an abortion?
After an abortion the body moves quickly through hormonal changes as pregnancy hormones fall and the menstrual cycle begins to reset. The most obvious shift is the drop in hCG as pregnancy tissue passes, followed by declines in estrogen and progesterone. Those decreases cause uterine bleeding, cramping, breast changes, and mood or energy shifts. Most hormone-related symptoms ease over several weeks as levels stabilize and your next period approaches. Understanding this process explains why some symptoms feel sudden at first and then gradually settle.
Ovarian Hormonal Stress Following Medical Abortion: A Study of Hormonal Status Abortion means ending a pregnancy, and that change brings measurable shifts in the body’s hormones. Early medical abortion — which uses medications to end a pregnancy — is generally seen as a conservative method, but the body does experience physiological stress as it stops preparing for gestation and lactation. Research on pituitary and ovarian changes after medical abortion is limited, which motivated our investigation. In this study we observed 50 women without contraindications to describe post-abortion hormonal status and related changes. OVARIAN HORMONAL STRESS AFTER MEDICAL ABORTION, NA Abenova, 2022
Which hormones change and what are their effects?
Human chorionic gonadotropin (hCG) falls quickly after pregnancy tissue leaves the body, signaling the end of pregnancy and triggering downstream hormonal adjustments. Estrogen and progesterone then decline, which reduces support for the uterine lining and causes bleeding and cramping; those drops also explain breast tenderness and shifts in mood or energy. Over several weeks hormone levels usually move back toward baseline, letting the hypothalamic-pituitary-ovarian axis reestablish regular cycles. Knowing which hormones shift helps explain why some physical and emotional reactions are strongest early in recovery and why the return of the menstrual cycle varies.
How does breast tenderness manifest post-abortion?
Breast tenderness is common after an abortion because pregnancy hormones that prepared the breasts for lactation drop rapidly, and the breast tissue adjusts back toward its pre-pregnancy state. Sensations can range from mild soreness to fullness, and occasional leaking is possible but uncommon. Symptoms usually improve over days and resolve in a few weeks. Practical steps include wearing a supportive bra, using warm or cool compresses for comfort, and avoiding breast stimulation if you don’t want to provoke milk production. Seek care if you develop severe swelling, fever, or abnormal nipple discharge.
What emotional effects can occur after an abortion?
Emotional reactions after an abortion are varied and normal: people commonly feel relief, sadness, grief, guilt, anxiety, or a mix of responses as hormones change and they process the experience. The timing and intensity of feelings differ widely and depend on mental health before the procedure, available support, personal values, and the circumstances that led to the decision. Many people find emotions fluctuate over days to weeks and lessen over time with supportive conversations and self-care. Remember that there’s no single “right” response — and it’s okay to seek help if feelings are interfering with day-to-day life.
Psychological Coping During the Immediate Post-Abortion Period The time from the abortion procedure until bleeding stops is a period of both physical and emotional adjustment. During this phase, individuals may experience symptoms such as cramping, bleeding, and breast tenderness alongside emotions like relief, sadness, or worry. Giving accurate information and strong support during this immediate period helps people recover more smoothly. Psychological coping in the immediate post-abortion period, SJ Ratcliffe, 2014
What are the common emotional responses after abortion?
Common emotional responses include relief at ending an unwanted pregnancy, sadness or grief over the loss of a potential pregnancy, guilt or shame if cultural pressures are present, and anxiety about physical recovery or future fertility. These feelings often come in waves and may be triggered by reminders like seeing a baby or attending follow-up visits — and it’s normal to feel several things at once (for example, relief and sadness). Research shows people’s experiences vary; some have brief emotional upset while others find counseling helpful. Naming and acknowledging your feelings is a helpful first step toward coping and planning support.
How can you heal emotionally and cope with post-abortion feelings?
Emotional healing usually combines practical self-care, supportive people, and professional help if needed. Options that help include talking with trusted friends or a counselor, practicing grounding or mindfulness, journaling, and engaging in restorative activities. Peer support or structured counseling can reduce distress for many people. Partners and support people can be helpful by listening without judgment, helping with daily needs during recovery, and encouraging professional care when feelings feel overwhelming. If you have persistent depression, severe anxiety, or thoughts of self-harm, seek mental health support right away.
How can you manage post-abortion symptoms and care for your body?
Managing symptoms focuses on safe pain relief, controlling bleeding, preventing infection, and gradually returning to normal activities. At-home strategies that often help include using recommended over-the-counter pain medicines, applying heat to ease cramps, resting during heavy bleeding, and following hygiene guidance to lower infection risk. Slowly reintroduce exercise and work to avoid setbacks, and make a follow-up plan with a clinician or support service so any concerns can be addressed quickly. Clear guidance on tampon use, sexual activity, and wound care helps protect healing during the first weeks. For further reading, you can visit how long do you bleed after an abortion.
What are effective pain management and bleeding control methods?
Start with over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs) taken as directed to reduce cramping and inflammation; combine this with heat therapy and rest for extra relief. For bleeding, use pads rather than tampons for the recommended period to minimize infection risk, and keep an eye on volume and clot size to detect heavy bleeding. Non-medication approaches like staying hydrated, pacing activity, and lying down during strong cramps can help. If severe pain continues despite medication, seek medical evaluation. Keeping a simple log of bleeding and pain is useful to share with a clinician if needed.
Common safe pain-management steps you can try at home include:
Take OTC NSAIDs as directed to reduce cramping and inflammation.
Use heat: a warm compress or heating pad on the lower abdomen can ease uterine cramps.
Rest and pace activity: avoid strenuous exercise until bleeding and pain decrease.
These measures often offer meaningful relief and support recovery; contact a clinician if symptoms worsen.
What hygiene and activity guidelines should you follow after abortion?
Keep the vulvar area clean with gentle washing, avoid baths, swimming pools, and douching for the recommended time to lower infection risk, and use sanitary pads instead of tampons until advised otherwise. Wait to resume vaginal intercourse until your provider gives the go-ahead — commonly about one to two weeks — so the cervix can close and infection risk falls; when you do resume sex, use effective contraception if you want to avoid pregnancy. Return to exercise gradually: begin with light walks and increase activity as bleeding and pain permit, listening to your body to avoid pushing too soon. Book any recommended follow-up visits to confirm recovery and discuss contraception or other questions.
If you want extra guidance tailored to recovery and emotional support, Her Smart Choice offers clear, compassionate resources focused on post-abortion care. Their materials can help you plan follow-up, learn self-care steps, and find counseling referrals.
What are the signs of complications after an abortion and when should you seek help?
Knowing warning signs helps you act fast if infection, incomplete abortion, or dangerous bleeding occurs. Emergency red flags include fever over 100.4°F (38°C), foul-smelling vaginal discharge, severe or worsening lower abdominal pain not eased by medication, passing large tissue fragments with heavy bleeding, dizziness or fainting, and soaking through sanitary pads quickly. If you have any of these signs, get urgent medical evaluation or go to emergency care so complications can be treated. Clear thresholds and quick action reduce risk and speed safer recovery.
How can you recognize signs of infection or incomplete abortion?
Infection often shows as fever, chills, increasing abdominal pain, and a foul or unusual vaginal discharge — symptoms that typically get worse rather than better and may come with a general feeling of being unwell or a fast heart rate. Incomplete abortion may present as ongoing heavy bleeding, continued severe cramping beyond the expected timeframe, passage of tissue after the procedure, or rising hCG levels if tested. Comparing the expected pattern (gradual improvement) to warning signs (worsening or new systemic symptoms) helps you decide whether to seek clinical care. If infection or retained tissue is suspected, prompt evaluation and treatment are important to prevent complications.
Short-Term Physical and Psychological Sequelae of Abortion Background: Abortion can be associated with short-term physical and psychological consequences. This study examined those effects across different types of induced abortion in women attending medical centers in Shiraz, Iran. Methods: A cross-sectional sample included 437 pregnancies that ended in abortion, gathered from a larger group of deliveries during a 4-month period. Participants completed demographic questionnaires and the Mississippi Post-Traumatic Stress Disorder Scale (M-PTSD); results were analyzed using standard statistical methods. Short-term physical and psychological health consequences of induced and spontaneous abortion: a cross-sectional study., N Tayebi, 2021
Watch for these infection or incomplete-abortion signals:
Fever or chills: a sign of systemic infection that needs medical review.
Foul-smelling discharge: suggests infection and warrants prompt care.
Persistent or worsening pain: especially if not relieved by medications.
If you notice any of these, contact a healthcare provider for evaluation.
When is heavy bleeding an emergency after abortion?
Heavy bleeding is an emergency when it causes dizziness, fainting, or when you are soaking through more than two sanitary pads per hour for two consecutive hours. Passing large clots (about the size of a lemon or bigger) along with lightheadedness, weakness, or a racing heart also calls for immediate medical attention. If heavy bleeding happens, lie down and, if possible, elevate your feet, call emergency services or go to urgent care, and bring someone with you if you can. After stabilization, clinicians will check for retained tissue, uterine atony, or other causes and arrange treatment that may include medication or procedures.
How does abortion affect fertility and future pregnancy planning?
Most people do not experience long-term infertility after an abortion. Fertility often returns quickly because ovulation may resume within weeks, so pregnancy is possible before your first post-abortion period. Many people get their next period around 4–6 weeks, though timing varies with prior cycle regularity, the abortion method, breastfeeding, and individual hormone recovery. If you want to avoid pregnancy, planning contraception right after the procedure is important since fertility can return fast; many methods can be started immediately depending on local guidance. If you plan to try for pregnancy later, waiting until you feel physically and emotionally ready — and confirming recovery with a clinician if advised — supports healthier planning.
Below is a concise comparison of common contraceptive options, suggested start timing after abortion, and key points to consider when choosing.
Contraceptive Option
When to Start Post-Abortion
Notes / Considerations
Combined oral contraceptive pill
Often can start immediately
Requires adherence; may increase bleeding initially
Progestin-only pill / injection
Can often start immediately
Good option if estrogen is contraindicated
Intrauterine device (IUD)
May be inserted at procedure or after confirmation
Offers long-term protection; immediate-start IUDs available in some settings
Implant
Can often start immediately
Highly effective, long-acting option
Condoms
Use immediately
Protects against pregnancy and STIs; user-dependent
This table makes it easier to compare options and choose what fits your needs; individualized counseling is helpful to match a method to your medical history and preferences. For guidance on choosing contraception or planning your next pregnancy, Her Smart Choice provides empathetic, plain-language resources to help you make an informed decision.
When does your menstrual cycle return after abortion?
Your period usually returns in about 4–6 weeks after an abortion for many people, but timing varies depending on how quickly ovulation resumes and how your hormones recover. Factors that affect return include previous cycle regularity, the abortion method, breastfeeding, and individual hormone patterns; some people get their next period sooner, others later. Tracking changes like shifts in cervical mucus, basal body temperature, or bleeding patterns can help you know what to expect after your abortion and inform contraception or pregnancy planning. If your period is much later than expected, check with a clinician for evaluation and reassurance.
What birth control options are recommended post-abortion?
Choosing contraception after abortion depends on personal preferences, medical history, and whether you want immediate protection. Many methods can be started right away to prevent a rapid return to fertility. Long-acting reversible options like IUDs and implants offer highly effective, low-maintenance protection and may be placed at the time of the procedure in some clinics. Pills, injections, and condoms are also valid immediate options depending on your needs. Discussing pros and cons — including side effects, reversibility, and how easy each method is to use — with a clinician or support resource helps you pick the best fit and start protection when you’re ready.
These steps help you get timely, effective pregnancy prevention that matches your preferences and health needs.
Frequently Asked Questions
What should I do if I experience severe pain after an abortion?
If severe pain doesn’t respond to over-the-counter pain medicines, seek medical attention. Intense pain can indicate complications such as infection or retained tissue. Monitor your symptoms closely; if pain gets worse or comes with fever or heavy bleeding, contact your healthcare provider right away for evaluation and possible treatment.
How can I support my emotional recovery after an abortion?
Emotional recovery combines self-care, social support, and professional help when needed. Try relaxation practices like mindfulness or journaling, and talk with trusted friends or family about what you’re feeling. If emotions become hard to manage, consider counseling or a support group. Remind yourself that a wide range of feelings is normal, and taking time to process them is an important part of healing.
Are there any dietary recommendations for recovery after an abortion?
A balanced diet supports recovery. Eat nutrient-rich foods — fruits, vegetables, whole grains, and lean proteins — to help your body replenish. Stay hydrated, especially if you experience bleeding. Iron-rich foods (for example, spinach and legumes) may help with fatigue related to blood loss. For personalized guidance, check with your healthcare provider.
When can I resume sexual activity after an abortion?
Most providers advise waiting about one to two weeks before resuming vaginal intercourse to reduce infection risk and allow the cervix to close; follow the specific guidance from your clinician. When you do have sex again, consider contraception if you want to prevent pregnancy, since fertility can return quickly.
What are the signs that I should seek medical help after an abortion?
Contact a provider if you develop fever over 100.4°F (38°C), foul-smelling vaginal discharge, severe abdominal pain that worsens, or heavy bleeding that soaks through more than two sanitary pads in an hour for two consecutive hours. These symptoms may signal complications that need prompt evaluation and treatment.
How can I track my recovery progress after an abortion?
Keep a simple journal of symptoms — note bleeding patterns, pain levels, and emotional changes. Record anything that feels unusual and bring those notes to follow-up visits. Tracking your menstrual cycle also helps you know when to expect your next period and assess overall reproductive health.
What resources are available for post-abortion support?
Resources include counseling services, support groups, and informational sites like Her Smart Choice. These can offer emotional support, practical advice, and referrals to care. Connecting with others who’ve had similar experiences can also be helpful. Don’t hesitate to reach out if you need support — you don’t have to go through recovery alone.
Knowing what to expect physically and emotionally after an abortion helps you manage recovery with greater confidence. By recognizing common symptoms, understanding hormonal changes, and using practical self-care strategies, most people navigate this period safely. For personalized support and clear resources tailored to your recovery, consider exploring Her Smart Choice’s guides and services. When you’re ready, reach out for the information and support that fit your needs.
Infection after an abortion happens when bacteria grow inside the uterus or nearby tissues following a medical or surgical procedure. Recovery varies: many people have expected bleeding and cramping that ease over days to weeks. This guide helps you tell routine recovery from infection and shows when to get medical care. You’ll find the most common warning signs, clear thresholds you can measure at home (for example, fever ≥100.4°F / 38°C or soaking pads), how symptoms may differ by procedure type, possible complications, and practical next steps for urgent care. The thresholds and recommendations here follow standard public-health guidance so you can act quickly and safely.
Most common warning signs of post-abortion infection
Post-abortion infection usually causes a mix of local uterine symptoms and systemic signs. Bacteria on retained tissue or introduced during a procedure can trigger inflammation, fever, and abnormal bleeding or discharge. Watch for measurable red flags that separate everyday recovery from infection: fever ≥100.4°F (38°C), bleeding that soaks many pads quickly, or a foul-smelling discharge. Catching infection early matters because untreated uterine infection can lead to endometritis or sepsis. Below is a short symptom list you can monitor at home, followed by a quick-reference table linking each sign to what to look for and what to do next.
Symptoms to watch for after an abortion include:
Fever of 100.4°F (38°C) or higher, especially if it won’t go away or comes with chills.
Heavy bleeding that soaks 2 or more pads per hour for two straight hours.
Foul-smelling vaginal discharge or gray/green tissue-like material.
Severe pelvic pain that gets much worse or won’t ease with your usual pain medicine.
Systemic signs like a fast heartbeat, lightheadedness, or fainting.
These signs suggest possible infection; the sections that follow explain each one and why it matters.
Quick-reference table: core symptoms, measurable thresholds, and the recommended action if you see them.
Symptom
Measurable Sign / Threshold
Recommended Action
Fever
Temperature ≥100.4°F (38°C), or persistent low-grade fever >48 hours
Call your provider the same day; seek urgent evaluation if you have chills or a very fast heartbeat
Heavy bleeding
Soaking ≥2 pads/hour for ≥2 hours or passing large clots >2 inches
Go to the emergency department or urgent care
Foul-smelling discharge
Strong, unpleasant odor; green/gray discharge or tissue-like clots
Contact your provider promptly for exam and possible antibiotics
Severe pelvic pain
Increasing pain not controlled by prescribed analgesics or sudden severe pain
Seek immediate in-person assessment; imaging may be needed
Systemic signs
Lightheadedness, rapid heart rate >100 bpm, low BP symptoms
Treat as possible sepsis—call emergency services
If more than one of these signs appears, get care right away. The next sections explain each symptom in plain language and what it usually means.
How fever after abortion can signal infection
A fever after an abortion can mean your body is fighting an infection. A single temperature ≥100.4°F (38°C) or a fever that lasts more than 48 hours is concerning for bacterial infection rather than a normal inflammatory response. Accompanying symptoms—rigors, severe body aches, or worsening pelvic pain—raise the chance that the uterus is infected (endometritis). Retained tissue or bacteria introduced during a procedure can trigger this response. If your fever meets these thresholds or comes with other warning signs, contact your healthcare provider right away; antibiotics are often needed.
This leads into bleeding, which is another key measurable sign.
When heavy bleeding is a concern
Some bleeding after an abortion is expected as the uterus sheds tissue, but it becomes dangerous when it meets specific measurable criteria. If you’re soaking two or more standard pads per hour for two consecutive hours, passing clots about the size of a lemon or larger, feeling dizzy, or fainting, get emergency care. Heavy bleeding can happen with infection if products of conception are retained, but it can also indicate a separate urgent problem that needs immediate stabilization. If you meet these metrics or feel faint or lightheaded, go to the ER.
Knowing how to describe bleeding clearly helps when you call for help.
What foul-smelling discharge usually means
A strong, unpleasant vaginal odor—especially gray-green discharge or tissue-like material—often points to bacterial overgrowth or necrotic retained tissue in the uterus. Normal post-procedure bleeding may be brown or red with small clots and no strong smell. When the discharge is noticeably foul or changes color, it suggests infection such as endometritis. If you notice this, especially with fever or worsening pain, contact your provider for evaluation and likely antibiotics.
Changes in discharge often lead providers to examine you and consider imaging.
How to tell if abdominal pain and cramping suggest infection
Cramping and discomfort are normal after both medical and surgical abortion. Pain that steadily worsens, becomes sharp and localized, or doesn’t respond to usual pain medicines may signal infection or retained tissue. Infection-related pain is often constant, gets worse over time, and can come with fever or nausea. Localized tenderness or rebound pain may prompt an ultrasound to check for retained tissue or an abscess. Stop strenuous activity, take pain medicine as directed, and call your provider if the pain increases or comes with other warning signs.
Knowing the difference between expected cramping and concerning pain makes it easier to get care when needed.
Other systemic symptoms that suggest infection
When symptoms go beyond the pelvis, infection may be spreading. Watch for chills, persistent nausea or vomiting, a fast heart rate, dizziness, fainting, confusion, or low urine output—these can mean sepsis or serious systemic infection. If uterine symptoms occur alongside any of these signs, seek emergency care right away. Treatment for spreading infection usually includes IV antibiotics and close monitoring, so quick action is important.
Next, we explain how warning signs differ between medical and surgical abortion.
How warning signs differ between medical and surgical abortion
Warning signs vary by procedure because medical abortion uses medication over days to expel tissue, while surgical abortion is completed in clinic in one visit. Medical abortion often causes heavier bleeding and stronger cramping initially; infection risk rises if tissue is incomplete. Surgical abortion tends to have shorter, immediate bleeding and cramping after the procedure but carries a peri-procedural infection risk if bacteria are introduced or fragments remain. Comparing expected timelines and red flags helps you know what’s normal and what needs medical attention.
Below is a comparison table summarizing typical timelines and when symptoms suggest infection for each abortion type.
Abortion Type
Typical Timeline / Expected Symptoms
When Symptoms Suggest Infection
Medical abortion (mifepristone + misoprostol)
Bleeding/cramping peaks within 24–72 hours, tapering over 1–2 weeks
Continued heavy bleeding after 2 weeks, fever, or persistent tissue passage
Surgical abortion (in-clinic)
Immediate procedure-related cramping and light bleeding that decreases over days
Fever within days, increasing pain, or unusual discharge after initial recovery
Both types
Some spotting may last 2–4 weeks
Any fever ≥100.4°F, heavy bleeding metrics, or foul-smelling discharge
Incomplete abortion is a more common cause of infection after medical abortion, while surgical procedures carry peri-procedural infection risk. The next sections describe procedure-specific warning signs.
Infection signs specific to medical abortion
Medical abortion uses mifepristone and misoprostol to cause the uterus to expel tissue over several days. Expect heavy bleeding and strong cramping at first that usually eases within a week. Signs of possible infection include bleeding that doesn’t settle after the expected timeframe, fever, foul-smelling discharge, or persistent pregnancy symptoms that suggest retained tissue. Because the process can be gradual, follow-up with ultrasound or serial hCG testing may be recommended if symptoms persist. If you have prolonged heavy bleeding, fever, or abnormal discharge more than a few days after the initial expulsion, contact your provider.
Next, surgical abortion risks and signs are covered.
Infection risks and signs after surgical abortion
Surgical abortion involves instruments placed in the uterus and is usually done in a single visit. Immediate cramping and light bleeding are common and normally improve over days. Infection can occur if bacteria are introduced during the procedure or if fragments are left behind, causing fever, localized pain, or smelly discharge within days. Some providers give prophylactic antibiotics in certain situations to reduce risk. If you develop fever, worsening pain, or unusual bleeding after a surgical abortion, seek prompt in-person evaluation to check for retained tissue, uterine perforation, or endometritis.
Knowing these differences helps you set expectations for follow-up and encourages timely care when red flags appear.
Complications that can lead to infection
Certain complications create conditions where bacteria can grow—retained products of conception (incomplete abortion), uterine perforation, or instrument-related injury are common examples. These issues leave necrotic tissue or change uterine anatomy, making infection more likely. If you notice ongoing bleeding, severe or persistent pain, or abnormal discharge, your provider may order an ultrasound to look for a complication.
The table below outlines common complications, typical signs, and usual diagnostic or treatment steps.
Complication
Typical Signs
Diagnosis / Treatment Implication
Retained products of conception
Ongoing heavy bleeding, cramping, tissue passage, fever
Ultrasound evaluation; possible medical management or surgical evacuation (D&C)
Incomplete abortion
Continued pregnancy symptoms or rising hCG, persistent bleeding
Serial hCG or ultrasound; may require additional medication or procedure
Uterine perforation
Sudden severe pain, shoulder-tip pain, signs after instrumentation
Surgical assessment; possible repair and infection prevention
Procedural infection (endometritis)
Fever, foul discharge, pelvic tenderness
Clinical diagnosis; antibiotics and possible surgical removal of retained tissue
How retained tissue or incomplete abortion leads to infection
Retained tissue provides dead material and blood where bacteria can multiply, causing uterine inflammation, ongoing bleeding, and foul discharge. You might suspect retained tissue if bleeding does not decrease, pain continues or worsens, or pregnancy tests stay positive longer than expected. Providers commonly use pelvic ultrasound to look for retained products and may use serial quantitative hCG measurements in some protocols. Treatment can range from expectant or medical management to surgical evacuation (D&C). Prompt care lowers the risk of wider infection and helps protect future fertility.
Signs of sepsis and when it’s an emergency
Sepsis is a life-threatening reaction to infection that needs immediate treatment. Red-flag signs include very high fever, very fast heart rate (tachycardia >100 bpm), low blood pressure or lightheadedness, rapid breathing, and changes in mental status. If you suspect sepsis, call emergency services and get to a hospital quickly—treatment usually requires IV antibiotics, fluids, and close monitoring. Early recognition and rapid treatment save lives, which is why prompt evaluation for post-abortion warning signs is so important.
Knowing sepsis criteria helps you act quickly if systemic symptoms appear.
When to seek immediate medical attention
Deciding whether to watch and wait, call your clinic, or go to the emergency department depends on measurable thresholds and how symptoms cluster. Seek immediate care for any of the following: fever ≥100.4°F with chills, heavy bleeding that meets pad metrics, fainting or near-fainting, severe unrelenting pelvic pain, or systemic signs of sepsis. For concerning but non-emergency symptoms—low-grade fever, increased bleeding without signs of low blood pressure, or new malodorous discharge—contact your provider the same day for triage. The checklist below helps you prioritize and tells you what to report when seeking care.
Emergency (Go to ER / call emergency services): Unconsciousness, fainting, heavy bleeding (≥2 pads/hour × 2 hours), severe pain with lightheadedness, or sepsis signs.
Urgent (Contact provider same day): Fever ≥100.4°F without collapse, foul-smelling discharge, increasingly heavy bleeding, or worsening pain.
Non-urgent (Call for advice/monitor): Low-grade fever for <48 hours, mild increased cramping, or light spotting beyond expected duration.
This triage framework helps you choose the right level of care and leads into practical steps for contacting a healthcare team.
Urgent symptoms that need emergency care
Some symptoms can be immediately dangerous because they signal major blood loss or widespread infection. Urgent signs include passing large clots with dizziness, fainting, bleeding that soaks many pads quickly, severe abdominal pain with shock signs, or very high fever with confusion or trouble breathing. These conditions require fast stabilization in an emergency setting. If you have any of these signs, arrange safe transport and tell emergency staff your symptoms began after a recent abortion so they can triage and treat you appropriately.
Knowing these urgent thresholds reduces delays in life-saving treatment and prepares you to communicate clearly with providers.
How to decide when to contact your healthcare provider
If symptoms are concerning but not clearly life-threatening, follow a simple approach: check measurable thresholds (temperature, pads/hour), note how long it’s been since the procedure, and list any accompanying signs (odor, pain, dizziness). When you call, report exact temperature readings, how many pads you’ve soaked and over what time, the character of any discharge, and any systemic symptoms. This information helps triage nurses decide whether you need same-day evaluation, imaging, or immediate antibiotics. Many clinics offer telehealth triage to guide next steps—clear, objective reporting speeds up appropriate care and reduces worry.
If you prefer local in-person help, many community reproductive-health centers and regional clinics offer same-day triage, follow-up care, or referral to emergency services when needed.
How to prevent and manage post-abortion infections during recovery
Preventing infection combines simple hygiene, following your provider’s instructions, timely follow-up, and getting treatment if warning signs appear. These steps reduce bacterial growth and make it easier to spot retained tissue early. Key practices include washing hands before changing pads, avoiding intra-vaginal products or sex until cleared, finishing any prescribed medications, and attending scheduled follow-ups.
Practical steps to lower infection risk:
Keep the genital area clean and change pads regularly; avoid douching or tampons until your provider says it’s safe.
Rest and avoid heavy lifting for the timeframe your clinician recommends; follow any wound-care instructions.
Finish any prescribed antibiotic course and attend follow-up appointments or telehealth checks.
If indicated, get screened and treated for STIs, since co-infection can raise post-procedure infection risk.
These measures reduce the chance of infection and make it easier to notice problems early. Below is guidance on follow-up care.
Best practices to prevent infection after abortion
Prevention focuses on limiting bacterial exposure, confirming complete expulsion of tissue, and contacting care quickly if recovery changes. Practice strict hand hygiene, avoid internal vaginal devices or sex until cleared, and follow medication instructions carefully for medical abortion. Some clinicians recommend STI screening or prophylactic antibiotics in selected cases—discuss options with your provider. Regular follow-up, in person or by telehealth, helps confirm recovery and lets clinicians treat infection early if it develops.
Next, what to expect from proper post-abortion follow-up.
What proper post-abortion care and follow-up involve
Follow-up typically includes a check-in within 1–2 weeks to review bleeding, pain, and recovery. Your provider may do a pelvic exam, ultrasound, or serial pregnancy testing if needed. Telehealth visits are often used to triage symptoms and determine if in-person assessment is required; imaging is reserved for suspected retained tissue or persistent symptoms. If infection is suspected, clinicians will prescribe appropriate antibiotics and may arrange surgical management for retained tissue. Timely follow-up and treatment return most people to full health and reduce long-term risks.
Many community clinics and reproductive-health centers offer rapid follow-up, counseling, and referrals for in-person evaluation or medication management.
Frequently Asked Questions
What should I do if I experience symptoms of infection after an abortion?
If you have fever ≥100.4°F, heavy bleeding, foul-smelling discharge, or severe pelvic pain, seek medical attention promptly. For emergency signs like fainting, soaking through many pads quickly, or symptoms of sepsis, go to the emergency room right away. For worrying but non-emergency symptoms, call your healthcare provider the same day for guidance. Early care lowers the chance of complications. For more information on foul-smelling discharge, visit how to treat smelly discharge after abortion.
How can I tell normal recovery from signs of infection?
Normal recovery usually means cramping and bleeding that steadily improve. Infection may look like a persistent fever, heavy bleeding that soaks two or more pads per hour, foul-smelling discharge, or worsening pain. Use the measurable thresholds in this guide to help decide when to call for care.
Are there factors that raise the risk of infection after an abortion?
Yes. Retained products of conception, pre-existing infections, or complications during the procedure (for example, uterine perforation) increase infection risk. Skipping post-procedure care instructions or poor hygiene can also raise the chance. Knowing these factors helps you take preventive steps and monitor recovery closely.
How does follow-up care help prevent infections?
Follow-up lets providers confirm the uterus has emptied, check for symptoms that suggest infection, and treat problems early. A typical follow-up visit occurs within 1–2 weeks and may include an exam, ultrasound, or pregnancy testing. Early detection and treatment prevent worsening infection and protect health.
Can I prevent infections after an abortion, and how?
Yes. Good hygiene, changing pads regularly, avoiding douching or tampons until cleared, following post-abortion instructions, finishing prescribed medications, and attending follow-up visits all reduce infection risk. These steps help prevent bacterial growth and make complications easier to catch early.
What should I know about sepsis after an abortion?
Sepsis is a severe, life-threatening response to infection. Look for high fever, rapid heart rate, low blood pressure, confusion, or breathing difficulty. If you have these signs, seek emergency medical care immediately—early treatment is critical.
Does the type of abortion affect infection risk?
Yes. Medical abortions, which expel tissue over several days, can carry higher infection risk if tissue is retained. Surgical abortions may introduce bacteria during the procedure or leave fragments behind. Understanding these differences helps you know what to watch for and when to seek care.
How soon can infection develop after an abortion?
Infection can appear within days but sometimes surfaces weeks later; many cases show up in the first week when tissue or bacterial overgrowth causes inflammation. Factors that affect timing include retained tissue, pre-existing infection, or bacteria introduced during the procedure. Stay alert for fever, worsening pain, foul discharge, or heavy bleeding during the first few weeks and contact your provider if any occur.
Can you get an infection after a medical abortion?
Yes. Most medical abortions proceed without infection, but there’s a small risk—especially if the abortion is incomplete or there was an existing infection. Watch for prolonged heavy bleeding, worsening pain, fever ≥100.4°F, or malodorous discharge. If you suspect infection after a medical abortion, contact your provider. Treatment may include antibiotics and, if needed, surgical evacuation.
Local reproductive-health centers and pregnancy-resource clinics can often provide follow-up, counseling, and arrange urgent care when infection is suspected.
Act quickly: fever with systemic signs or heavy bleeding needs immediate care.
Prevention helps: good hygiene, avoiding intra-vaginal activity until cleared, following medications, and attending follow-up reduce risk.
This FAQ reinforces the practical thresholds to use when deciding whether to seek care.
Conclusion
Knowing the warning signs of infection after an abortion helps you get care quickly and protect your health. Monitor clear thresholds—fever, heavy bleeding, and foul-smelling discharge—and contact your provider when symptoms meet the criteria in this guide. Simple prevention steps and timely follow-up reduce risk. If you’re unsure or worried, reach out to a local reproductive health clinic for advice and support.
Declaration
This article has been researched, written, and verified by the Smart Choice Team based on established medical guidelines and public health standards concerning post-abortion care.
Vaginal discharge after an abortion is a normal part of healing: the uterus clears blood, tissue and mucus as it returns to its pre‑pregnancy state, producing different colors and textures over days to weeks. This guide explains what typical post‑abortion discharge looks like, how long common patterns usually last, and which changes suggest infection or other complications so you know when to seek care. At Her Smart Choice we aim to be a trusted medical resource — you’ll find a week‑by‑week view, practical monitoring steps, red‑flag lists, prevention and recovery tips, and concise answers to common questions about yellow or prolonged discharge. Recovery varies by procedure type and gestational age, so this article focuses on helping you spot healthy healing versus signs that need clinical evaluation, using clear examples, EAV‑style tables, and actionable checklists.
What Is Normal Vaginal Discharge After an Abortion?
Normal post‑abortion discharge is usually a mix of fresh blood, older clots and vaginal mucus that gradually thins and lightens as the uterus heals. This reflects uterine involution and shedding of the decidua and residual blood — early bleeding tends to be red or brown, while mucus‑like or clearer discharge appears later to help clear debris and support tissue repair. Expect volume and color to decline over days to weeks; most people notice the heaviest bleeding in the first week and steady reduction afterward. Knowing typical colors and textures makes it easier to spot changes that could indicate infection or retained tissue, so the next section breaks down common appearances and timelines.
Typical colors and consistencies follow predictable stages: brown or dark red often represents older blood clearing out during the first 1–2 weeks, pink spotting appears as bleeding tapers, and mucus‑like or whitish discharge is common as the lining repairs. Mild or no odor is usual; a strong, unpleasant smell is not. These baseline patterns help you monitor changes and decide when to follow up with a provider.
Discharge usually decreases most quickly in the first 2–4 weeks, though intermittent spotting or brown staining can persist for some people up to 6–8 weeks. Duration varies with whether the abortion was medical or surgical, gestational age, and individual healing. If bleeding increases after initial improvement or heavy bleeding resumes, contact your clinician for reassessment. Below is a concise EAV‑style table summarizing common colors and what they commonly mean.
Color / Type
Typical Consistency & Odor
Likely Meaning / Recommended Action
Bright red blood
Thin blood, occasional clots, minimal odor
Active bleeding common in the first few days; monitor volume and contact your provider if you’re soaking a pad in an hour
Brown or dark red
Thick, older blood, little to no odor
Normal as the uterus clears older blood; expect intermittent spotting for several weeks
Pink or light spotting
Thin, light flow
Normal as bleeding tapers; resume usual activities gradually as advised
Clear/white mucus
Watery or mucus‑like, odorless
Normal healing discharge that signals lining remodeling
If your experience matches these patterns, healing is likely progressing. The next section explains how to recognize abnormal discharge and clear red flags that need prompt attention.
Common Colors and Consistencies Seen in Normal Recovery
Normal discharge typically starts bright red in the immediate days after the procedure, then shifts to brown and later to clearer, mucus‑like fluid as healing continues. Bright red usually means fresh bleeding from the uterine lining; brown indicates older blood being expelled. Later, whitish or clear mucus without a strong odor usually signals the cervix and uterus returning to baseline and often coincides with less cramping and lighter flow. Noticing these textures and colors helps you tell routine recovery apart from signs that need a clinical check.
Changes in consistency and color are influenced by hormones and the procedure type: some surgical procedures may show a faster drop in bleeding for some people, while medical abortions can cause longer spotting. If the discharge becomes thick, pus‑like, green or gray, or if you develop new systemic symptoms, treat it as potentially abnormal and see the section on infection signs below.
How Long Does Normal Discharge Last After an Abortion?
Most people have the heaviest bleeding in the first 1–3 days, with a noticeable reduction by 2–4 weeks and possible intermittent spotting that can last up to 6–8 weeks. The process reflects gradual uterine contraction and endometrial repair; larger gestations and retained tissue can prolong bleeding. Individual factors — clotting differences, prior infections, and the abortion method — affect timing, so use these timelines as general guidance rather than strict rules. A steady trend of improvement is reassuring; worsening color, increasing volume, or new symptoms should prompt evaluation. For more information, see our comprehensive guide on managing post-abortion bleeding.
Keep scheduled follow‑ups and communicate with your provider if you have concerns. Noting color, amount, smell and symptoms like cramping or fever makes triage faster and more accurate. If your recovery shows steady improvement, continue routine self‑care; if not, use the monitoring checklist later to prepare for a clinical call.
A simple self‑assessment framework helps patients track expected recovery patterns after abortion.
Post‑Abortion Care: A Framework for Patient Self‑Assessment The method compared outcomes of discharged post‑abortion patients to create self‑assessment tools that guide follow‑up and clarify common recovery responses.
How Can You Identify Abnormal Discharge and Signs of Infection After Abortion?
Discharge that is foul‑smelling, green or gray, thick and pus‑like, or accompanied by systemic symptoms such as fever or severe pain often indicates infection or retained tissue. Bacterial overgrowth or inflammation produces purulent material and can trigger systemic responses — these conditions usually need prompt clinical assessment and often antibiotics or a procedure. Early recognition of red flags improves outcomes and reduces the risk of serious complications like sepsis. The list below highlights the visual and systemic warning signs and the immediate actions to take. You can learn more about vaginal discharge for additional insights.
Foul‑smelling vaginal discharge or a new, strong unpleasant odor — a sign of bacterial infection.
Green, gray, or pus‑like discharge that is thicker than earlier mucus‑like drainage.
New or worsening fever above 100.4°F (38°C), chills, or flu‑like symptoms suggesting systemic infection.
Severe, continuous lower abdominal pain or heavy bleeding (soaking a pad in an hour) that could indicate retained tissue or hemorrhage.
These signs often appear together; for example, foul odor plus fever strongly suggests infection and needs urgent assessment. If you notice any combination of these symptoms, seek medical evaluation promptly — the next subsection describes how infected discharge typically looks and smells to help you decide when to call.
What Does Infected Discharge Look and Smell Like?
Infected discharge is commonly thick and discolored — yellow, green or gray — and usually has a noticeably foul or fishy odor, reflecting bacterial overgrowth or necrotic tissue. It may increase in volume and be accompanied by pelvic pain and tenderness. Typical causes include uterine infection from retained tissue or ascending bacteria after the procedure. Recognizing these visual and olfactory cues helps you prioritize medical contact when infection is suspected.
If infected discharge comes with systemic signs such as fever, chills or severe cramping, treat it as urgent and seek clinical care immediately. The following section lists other non‑discharge symptoms that often accompany infection and explains urgency levels for contacting a provider.
What Other Symptoms Indicate Post‑Abortion Infection?
Non‑discharge symptoms that commonly point to infection include fever over 100.4°F (38°C), persistent or worsening pelvic pain, dizziness or fainting, nausea or vomiting, and heavy bleeding with large clots. These signs reflect the immune system reacting to bacterial invasion or retained products of conception and can progress quickly without treatment. Use severity mapping: high fever, fainting, or heavy bleeding with signs of shock requires emergency care, while low‑grade fever or increasing pain usually warrants same‑day clinic evaluation. Monitoring symptom clusters and how they change helps decide whether to call your clinic or go to the emergency department.
Keep a brief symptom diary with temperature, pain level, bleeding amount and discharge details; this record helps clinicians triage and decide on interventions like antibiotics or further procedures. The next section groups discharge types and their most likely causes to help with decision‑making.
What Are the Different Types of Post‑Abortion Discharge and What Do They Mean?
Discharge can be grouped by color and consistency to suggest the most likely cause — from normal healing (brown or pink) to infection (green, gray, pus‑like) or retained tissue (heavy bleeding with clots). Underlying mechanisms include breakdown of blood products, mucosal repair, bacterial growth, or incomplete uterine evacuation. Mapping what you see to likely diagnoses helps target follow‑up and improves communication with clinicians. Below is an EAV‑style table pairing common appearances with probable causes and recommended actions.
Appearance
Key Attributes
Differential Diagnosis / Recommended Action
Brown or dark red
Thick, older blood, low odor
Normal healing; monitor and follow up if persistent >8 weeks or if it worsens
Pink/light spotting
Thin, scant flow
Normal tapering bleeding; rest and routine monitoring
Yellow/green/gray
Thick, discolored, often foul odor
Possible bacterial infection; contact your provider for evaluation and likely antibiotics
Heavy bleeding with clots
Large volume, passing clots, dizziness
Possible retained tissue or hemorrhage; seek immediate medical care
This mapping helps you decide when to monitor at home versus when to seek evaluation; act promptly if discharge suggests infection or if bleeding is heavy. The next subsections explain common normal colored discharge and when colored discharge becomes concerning.
What Does Brown or Pink Discharge After Abortion Mean?
Brown discharge usually represents older blood being expelled during uterine healing and is common in the first several weeks. Pink spotting is lighter and signals that fresh bleeding is tapering as the endometrium repairs. If these patterns are steady or improving, watch and wait is appropriate; but if brown or pink discharge comes with fever, worsening pain, or a sudden increase in bleeding, it could indicate retained products of conception or infection and should be evaluated. Tracking the trend and any associated symptoms helps decide whether clinical follow‑up is needed.
Is Yellow, Green, or Gray Discharge After Abortion a Cause for Concern?
Yellow, green or gray discharge is more likely to indicate infection when it is thick, persistent and has a foul odor, or when it is accompanied by fever or pelvic pain. Bacterial colonization or retained tissue can create purulent material and systemic symptoms that need antibiotics or procedural care. If such discharge appears but is mild, odorless and decreasing over 24–48 hours, close monitoring may be reasonable; any worsening or new systemic signs means contact your provider right away. Early treatment typically involves antibiotics aimed at common uterine pathogens and assessment (including ultrasound if indicated) to check for retained tissue.
The next section offers practical steps to reduce infection risk and support recovery after an abortion.
How Can You Prevent Infection and Support Healing After an Abortion?
Practical steps reduce the risk of post‑abortion infection by limiting bacterial exposure and supporting the body’s recovery. The basic idea is to avoid practices that introduce bacteria into the vagina or uterus, and to support immune function with good nutrition, rest and emotional care. Below are hygiene do’s and don’ts, lifestyle tips for recovery, and an evidence‑informed approach to emotional wellbeing.
Hygiene and activity guidance centers on avoiding intra‑vaginal products and keeping the external genital area clean and dry. The list below summarizes clear, actionable hygiene steps for recovery.
Avoid intra‑vaginal products such as tampons, douches and menstrual cups until your provider clears you.
Use sanitary pads rather than internal products and change them often to limit bacterial growth.
Keep the external genital area clean and dry; wash gently with mild soap and water and avoid scented products or baths if your provider advises against them.
What Hygiene Practices Help Prevent Post‑Abortion Infection?
Avoiding douching, tampons and sexual intercourse for the provider‑recommended interval helps prevent ascending infections by keeping the cervical canal protected from external bacteria. Change pads frequently and wear breathable cotton underwear to reduce moisture that fosters bacterial growth. Practice careful hand hygiene before and after pad changes or personal care. If your clinician prescribes antibiotics or other instructions, follow them exactly. These precautions, combined with symptom monitoring, form the foundation of safe aftercare.
How Do Rest, Nutrition, and Emotional Well‑Being Support Recovery?
Rest and graded activity support uterine involution and can reduce bleeding; avoid heavy lifting and strenuous exercise in the immediate recovery period s/o your body can focus on repair. Nutrition — including iron‑rich foods, adequate protein and plenty of fluids — replenishes losses from bleeding and supports immune function. Sleep promotes overall healing and hormone balance. Emotional wellbeing matters because stress can heighten pain and slow recovery; reach out to friends, family or a counselor if you need support. Combining physical and emotional self‑care helps speed recovery and lowers the chance of complications.
Practical examples: gentle walking as tolerated after 24–48 hours, prioritizing iron and protein if bleeding was heavy, and contacting a clinician or support resources for persistent anxiety or depressive symptoms. The next section explains when to contact a doctor about discharge concerns, with clear warning signs.
When Should You Contact a Doctor About Discharge After an Abortion?
Contact a doctor when discharge is paired with systemic symptoms (fever, severe pain), when bleeding is heavy or getting worse, or when discharge becomes foul‑smelling, green/gray or pus‑like. These findings can signal infection, retained tissue or hemorrhage — conditions that may require antibiotics or immediate procedural care. Prioritizing these signs ensures timely treatment and lowers the risk of serious complications. The table below lists common symptoms, urgency levels and recommended immediate actions.
Symptom / Finding
Characteristic
Urgency / Recommended Action
High fever (>100.4°F / 38°C)
Systemic sign, may include chills
Urgent: contact your provider right away or go to the ER if severe
Foul‑smelling or green/gray discharge
Thick, purulent odor
Urgent: contact the clinic same day for antibiotics and evaluation
Heavy bleeding (pad soaked in ≤1 hour)
Large volume, clots, lightheadedness
Emergency: go to the ER or call emergency services immediately
Mild spotting without fever
Light, decreasing flow
Routine: monitor and follow up at your scheduled visit
This checklist clarifies which situations need emergency care versus same‑day clinic evaluation; acting according to these categories helps keep you safe. The next two subsections expand on absolute emergency signs and offer practical monitoring strategies for home use.
Warning Signs That Require Immediate Medical Attention
Seek emergency care for heavy bleeding that soaks a pad in an hour or less, passing very large clots, fainting or near‑fainting, sustained high fever above 100.4°F (38°C), or severe continuous abdominal pain not relieved by pain medication. These signs can indicate hemorrhage, sepsis, or retained tissue with acute infection and require immediate transport to an emergency department. Concrete examples — such as soaking two pads in an hour or feeling dizzy when standing — help you recognize severity quickly. If you have any of these signs, get emergency help without delay.
When you arrive, telling staff the amount of bleeding, how long you’ve had a fever, and whether you felt faint can speed triage and treatment. The following subsection gives a simple monitoring checklist to help you decide when to call your clinician before symptoms escalate.
How to Monitor Discharge Changes and Know When to Seek Help
A straightforward monitoring routine improves accuracy when assessing discharge and communicating with clinicians: note color, amount (light/moderate/heavy), odor, and associated symptoms like fever or pain, and record the date and time of any notable changes. If discharge worsens over 24–48 hours, if a new foul smell or green/gray color appears, or if systemic symptoms develop, contact your provider promptly — sooner if you have a fever or heavy bleeding. When calling, use concise phrases like: "I have green, foul‑smelling discharge for 12 hours and a fever of 101°F." That helps clinicians triage correctly. Keeping a brief diary and using clear language speeds evaluation and improves care decisions.
Monitoring empowers you to act early and gives clinicians the information they need to recommend antibiotics, imaging, or in‑person assessment. The next section answers common patient questions about yellow discharge and prolonged bleeding.
Common Questions About Post‑Abortion Discharge
People often ask whether yellow discharge is normal and how long discharge can last. Short, evidence‑based answers help set expectations and reduce anxiety. The Q&A below gives direct guidance, clear qualifiers and sample phrases to use when contacting your clinician.
Is Yellow Discharge Normal After an Abortion?
Yellow discharge can be normal if it’s light, odorless and gradually decreasing — it may be old blood mixed with mucus as the lining heals. However, yellow discharge that is thick, foul‑smelling, or accompanied by fever or worsening pain is more likely to be an infection and needs prompt evaluation. If you’re unsure, monitor closely for 24–48 hours; any progression to a foul smell, a change toward green/gray, or new systemic symptoms should prompt a call to your provider. This approach balances reassurance for mild changes with clear escalation criteria for infection.
Can Discharge Last for Several Weeks After an Abortion?
Yes — intermittent spotting or brown discharge can continue for several weeks, sometimes up to 6–8 weeks, particularly after medical abortion or later gestations. This reflects ongoing uterine healing and gradual clearance of blood. Factors that prolong discharge include retained tissue, infection, and individual variation in uterine involution. Persistent worsening or new red‑flag symptoms should prompt evaluation. Track trends: steady improvement is reassuring, while increasing volume, a color change to green/gray, or new fever is not.
This guide gave practical timelines, visual cues, EAV‑style tables, prevention steps, monitoring checklists, and clear red‑flag criteria so you can tell normal recovery from issues that need care. Use the symptom descriptions and sample phrases here when contacting your clinician to help them assess urgency and plan next steps.
Frequently Asked Questions
What should I do if I notice a sudden increase in bleeding after an abortion?
If bleeding suddenly becomes heavier — especially if you’re soaking through a pad in an hour or less — seek medical attention immediately. This can indicate retained tissue or hemorrhage and may require urgent treatment. Watch for dizziness, severe pain or large clots, and call your healthcare provider or go to the ER right away if you have these signs.
How can I differentiate between normal and abnormal discharge after an abortion?
Normal discharge typically includes blood, mucus and tissue that changes over time: bright red early on, then brown or pink, and later clearer or whitish. Abnormal discharge is often thick, foul‑smelling or green/gray and may come with fever or severe pain. Tracking color, odor and volume helps you identify concerning changes that warrant medical attention.
Is it normal to have cramping along with discharge after an abortion?
Mild cramping is common as the uterus contracts to heal and return to its pre‑pregnancy size. However, if cramping becomes severe, or occurs with heavy bleeding, fever or foul‑smelling discharge, contact your healthcare provider. Monitoring how intense and how long cramps last helps determine whether they’re within the expected range.
What lifestyle changes can support recovery after an abortion?
Support recovery with a balanced diet rich in iron and protein, plenty of fluids, and restful sleep. Avoid heavy lifting and strenuous exercise for a few days, use sanitary pads instead of tampons, and practice good hygiene. Emotional support — from friends, family or counseling — can also improve recovery and help manage stress or anxiety. For more information, check out our what to eat after abortion for fast recovery.
How can I track my recovery progress after an abortion?
Track recovery by noting discharge color, consistency and volume, and any symptoms like cramping or fever. A simple diary with dates and brief notes is useful for discussions with your provider. Look for a gradual decrease in bleeding and improvement in symptoms; sudden changes or worsening signs should prompt medical advice. Keep follow‑up appointments as recommended.
When is it safe to resume sexual activity after an abortion?
Most providers recommend waiting at least two weeks before resuming sexual activity, or until your clinician clears you. This gives your cervix time to close and lowers infection risk. If you notice unusual discharge, pain, or other concerning symptoms, check with your provider before having sex. Talk openly with your partner about timing and comfort when you’re ready to resume intimacy.
Conclusion
Knowing the usual patterns of vaginal discharge after an abortion helps you recognize healthy recovery and identify possible complications. Monitor changes in color, consistency and associated symptoms so you can get timely care when needed. Empower yourself with this information and take practical steps to support healing. For more resources and guidance on post‑abortion care, explore our other articles and clinical resources.
The birth control pill is a daily oral hormonal contraceptive that prevents pregnancy by changing normal reproductive processes. This FAQ breaks down how pills work, the main formulations, benefits beyond pregnancy prevention, common side effects and rare but serious risks, and practical steps to match pill choices to your health goals and lifestyle. Many people want straightforward, evidence-based answers about effectiveness, side effects, drug interactions, and how to pick a pill that fits their medical history and routine. Here you’ll find clear explanations, comparison tables, and checklists you can use when talking with your clinician—covering mechanism of action, pill types, non-contraceptive benefits, safety considerations, and quick answers to common concerns like missed doses, mood changes, and weight.
What Are Birth Control Pills and How Do They Work?
Birth control pills are oral medications that contain hormones—either both estrogen and a progestin (combined pills) or progestin alone (mini‑pills). They prevent pregnancy mainly by suppressing ovulation, thickening cervical mucus so sperm can’t reach an egg, and thinning the uterine lining to make implantation less likely. Combined and progestin‑only pills differ in hormone type and how sensitive they are to timing, which affects side effects and who can safely use them. Knowing these mechanisms explains why taking pills consistently and avoiding interacting medicines matters for effectiveness, and why certain health conditions rule out estrogen‑containing options. Our goal is to give clear, practical information so you can make confident, informed decisions about contraception.
What Hormones Are in Birth Control Pills and Their Roles?
Pills use two hormone classes: estrogen (commonly ethinyl estradiol) and synthetic progestins. Estrogen helps keep periods regular and supports ovulation suppression but also raises clotting risk in some people—an important factor when prescribing for smokers or older users. Progestins thicken cervical mucus to block sperm and thin the uterine lining; at higher doses or in certain formulations they may also suppress ovulation. Different progestins vary in androgenic or anti‑androgenic activity, which is why some pills can improve acne or influence mood differently from others. mood swings
How Do Birth Control Pills Prevent Pregnancy?
Pills reduce the chance of conception through three complementary actions. First, they suppress ovulation so an egg is not released. Second, they thicken cervical mucus, making it hard for sperm to move and survive. Third, they thin the endometrium, lowering the likelihood that a fertilized egg would implant. These layers of protection work best with correct use; missed pills, vomiting, diarrhea, or certain medications can weaken one or more mechanisms—so it’s important to know missed‑pill rules and interaction risks.
What Are the Different Types of Birth Control Pills?
Oral contraceptives fall into two main groups: combination pills (estrogen plus progestin) and progestin‑only pills. Within combination pills you’ll find monophasic formulations (same hormone dose each active pill), multiphasic packs (dose varies across the cycle), and extended‑cycle or continuous regimens that cut down or eliminate monthly withdrawal bleeds. Progestin‑only pills contain no estrogen and are often chosen for people who are breastfeeding or who have contraindications to estrogen, but they require stricter timing for reliable protection. Knowing these categories helps you match a clinical goal—acne control, lighter periods, breastfeeding compatibility—to the right formulation.
Pill Type
Hormone Content / Cycle Type
Typical Use / Advantage
Monophasic combination
Estrogen + progestin; same dose daily
Simpler routine and predictable bleeding control
Multiphasic combination
Estrogen + progestin; varying doses across pack
Designed to mimic natural hormone shifts; may reduce some side effects for a few users
Extended-cycle combination
Estrogen + progestin; 91-day or continuous regimens
Fewer withdrawal bleeds—helpful for heavy periods or endometriosis
Progestin-only (mini-pill)
Progestin only; taken daily at the same time
Good for breastfeeding or estrogen contraindications; timing-sensitive
This table summarizes how formulations differ and where they’re most useful—use it to narrow options before you talk with your clinician. Clear, practical information helps people choose a pill that fits both health needs and lifestyle.
What Are Combination Pills and Their Variations?
Combination pills pair estrogen with a progestin and come in monophasic, multiphasic, and extended‑cycle formats that change hormone exposure and bleeding patterns. Monophasic packs give a steady hormone dose each active day, which simplifies tracking side effects and cycle control. Multiphasic packs vary doses across the pack to more closely resemble natural fluctuations; some users find reduced breakthrough bleeding, though major advantages over monophasic pills are limited. Extended‑cycle regimens reduce or stop monthly withdrawal bleeds, which can improve quality of life for people with heavy periods or endometriosis.
What Are Progestin-Only Pills and Who Should Use Them?
Progestin‑only pills work mainly by thickening cervical mucus and, in some formulations, by suppressing ovulation. They’re a preferred option when estrogen is contraindicated—such as during breastfeeding or for people at higher clotting risk. A key limitation is strict timing: many mini‑pills must be taken within the same 3‑hour window each day to remain effective, so consistent routine and adherence are essential for dependable protection.
Progestin-Only Pills for Contraception: Efficacy and Acceptability This review compared progestin‑only oral contraceptives—administered continuously and without estrogen—to combined oral contraceptives. Randomized trials were examined to assess differences in effectiveness, acceptability, and continuation rates, but comparative conclusions remain limited by available data. Progestin‐only pills for contraception, 2010
A systematic review summarized continuous use of progestin‑only pills and highlighted the need for more head‑to‑head studies comparing them to combined options.
A New Progestin-Only Pill Containing Drospirenone: Efficacy and Safety Hormonal contraceptives are effective and generally safe for preventing pregnancy. Progestins are used in combined methods and as sole agents in progestin‑only pills, implants, intrauterine systems, and injections. Newer estrogen‑free progestin‑only formulations—such as a 4 mg drospirenone pill—offer ovulation inhibition with anti‑androgenic and anti‑mineralocorticoid actions and have been authorized in multiple regions. Oral progestins in hormonal contraception: importance and future perspectives of a new progestin only-pill containing 4 mg drospirenone, 2021
Recent progestin‑only options, including drospirenone formulations, expand estrogen‑free choices with promising efficacy and tolerability profiles.
What Are the Benefits of Taking Birth Control Pills?
Beyond strong contraceptive protection, birth control pills can improve everyday health and long‑term outcomes. They can make periods more predictable, ease menstrual cramps and reduce blood loss, help clear acne for many users, and treat conditions such as PCOS and endometriosis. Long‑term use is linked to lower ovarian and endometrial cancer risk, while evidence for other long‑term effects varies by formulation. Knowing how each benefit happens helps set realistic expectations for when and how much improvement to expect.
Benefit
Mechanism
Typical Onset / Evidence Strength
Menstrual regulation
Hormone cycle control and endometrial stabilization
Weeks to months; strong clinical evidence
Reduced dysmenorrhea
Lower prostaglandin-driven bleeding and thinner lining
Weeks; moderate–strong evidence
Acne improvement
Anti‑androgenic progestins and reduced ovarian androgen production
2–6 months; moderate evidence
Reduced ovarian/endometrial cancer
Suppressed ovulation and endometrial thinning
Years of use; strong epidemiological evidence
The table ties each benefit to its hormonal mechanism and typical timeline, helping you weigh likely outcomes when choosing a pill.
How Effective Are Birth Control Pills at Preventing Pregnancy?
With perfect use, combination pills are about 99% effective; with typical use they’re closer to 91% because missed doses and timing lapses occur. “Perfect use” means taking the pill daily at the same time and avoiding interacting medications; “typical use” reflects real‑world adherence where missed pills and late doses reduce protection. Factors that lower effectiveness include missing multiple pills, taking enzyme‑inducing drugs, vomiting or prolonged diarrhea, and inconsistent timing for progestin‑only pills. Those numbers help explain why adherence and understanding interactions are so important.
What Non-Contraceptive Benefits Do Birth Control Pills Offer?
Many users gain symptom relief and longer‑term health advantages from hormonal contraception. Combined regimens and extended‑cycle options can reduce heavy or painful periods by limiting endometrial buildup. Pills with anti‑androgenic progestins commonly improve acne over several months. Epidemiological studies also show reduced ovarian and endometrial cancer risk with longer use—an important factor when weighing benefits against risks. These non‑contraceptive effects often guide the choice of formulation based on personal health goals.
Mechanism of Action of Progestin-Only Oral Contraceptives Progestin‑only oral contraceptives primarily prevent pregnancy by producing cervical mucus that is hostile to sperm, which reduces the chance of fertilization. This cervical mucus effect is a central mechanism for these agents. The mechanism of action of hormonal contraceptives and intrauterine contraceptive devices, 1999
For progestin‑only pills, the hostile cervical mucus is a key way they stop sperm from reaching an egg and thus prevent pregnancy.
What Are the Common Side Effects and Serious Risks of Birth Control Pills?
Most side effects are mild and improve within a few months as your body adjusts; serious complications are uncommon but important to recognize. Early side effects often include nausea, spotting between periods, breast tenderness, and short‑term headaches—many of which resolve after 2–3 cycles or after switching formulations. Rare but serious risks include venous thromboembolism (DVT or PE), stroke, and heart attack—risks that are mainly linked to estrogen‑containing pills in people with specific risk factors. Identifying higher‑risk individuals—like smokers over 35, people with a history of clots, or those with certain migraine types—helps guide safer prescribing.
Common side effects and basic management tips:
Nausea: Try taking the pill with food or at bedtime; reassess after 1–2 cycles.
Spotting or breakthrough bleeding: Often settles on its own; consider a different formulation if it persists beyond three cycles.
Breast tenderness: Usually temporary; lower‑estrogen options may help if it continues.
Headaches and mood changes: Track timing and severity; see a provider if symptoms are new, severe, or worsening to review options.
Risk/Side Effect
Likelihood
Who's at Higher Risk
Nausea, spotting, breast tenderness
Common; often transient
New users and those starting higher estrogen doses
Blood clots (DVT/PE)
Rare; combined pill ~3–9 per 10,000 woman‑years
Smokers >35, prior clot history, thrombophilia
Stroke / MI
Very rare in young healthy non‑smokers
Smokers, uncontrolled hypertension, older age
Cancer risks (breast/cervical)
Small absolute increase or neutral
Varies; benefits include reduced ovarian/endometrial risk
Use this risk summary to guide a focused conversation with your clinician about which risks are most relevant to you.
What Are the Most Common Side Effects of Birth Control Pills?
Common side effects typically appear in the first few cycles and then often fade as hormone levels stabilize. Nausea usually improves with food or evening dosing; spotting or irregular bleeding often resolves after two to three cycles or when switching formulations. Breast tenderness and mild headaches are common and usually temporary. Mood effects vary—some users feel better, others notice worsening mood—so monitor changes closely during the first months and discuss alternatives with your provider if problems persist.
What Serious Health Risks Are Associated with Birth Control Pills?
Serious risks are uncommon but clinically meaningful. Estrogen‑containing pills raise the relative risk of venous thromboembolism, but the absolute risk remains low for most young, healthy, non‑smokers. The greatest increases in clot risk occur in smokers over 35 and people with a personal or strong family history of clotting disorders; these groups are often advised to avoid combined pills. Stroke and heart attack are rare in young healthy individuals but rise with traditional cardiovascular risk factors like hypertension, smoking, and older age. The cancer risk profile is mixed: ovarian and endometrial cancer risk is reduced with pill use, while small, variable effects on breast and cervical cancer have been reported—these trade‑offs should be discussed individually with a clinician.
How Do You Choose the Right Birth Control Pill for Your Needs?
Choosing the right pill means matching your medical history, lifestyle, and health priorities to pill characteristics in a clear, patient‑centered way. Start by listing absolute and relative contraindications—smoking status, age, clotting history, migraines with aura, and blood pressure—that may rule out estrogen‑containing options. Then align goals (acne control, fewer periods, breastfeeding) with pill types: anti‑androgenic combination pills for acne, extended‑cycle regimens for heavy or painful periods, and progestin‑only options when estrogen isn’t appropriate. This process helps prepare for a productive shared decision with your clinician.
Decision checklist (begin here when preparing to consult a clinician):
Medical contraindications: Note smoking status, age, any clotting history, migraine type, and blood pressure.
Lifestyle factors: Consider your ability to take a daily pill on time, desire for fewer periods, and breastfeeding plans.
Health goals: Prioritize acne reduction, menstrual control, PCOS management, or minimizing side effects.
Medication review: List enzyme‑inducing drugs or other medicines that could lower contraceptive levels and discuss alternatives.
This checklist supports shared decision‑making with your provider and highlights safety and adherence factors that usually determine the best option.
What Medical and Lifestyle Factors Affect Birth Control Pill Choice?
Several medical and lifestyle details guide which pill is safest and most effective for you. Key medical factors include prior blood clots, smoking combined with age over 35, uncontrolled hypertension, and migraine with aura—conditions that typically rule out estrogen‑containing pills. Lifestyle factors include whether you can take a pill at the same time every day (especially important for progestin‑only pills), travel or work schedules that affect timing, and whether you want to reduce or skip monthly bleeding. Medication interactions—particularly enzyme‑inducing drugs—can lower hormone levels, so a full medication review is essential when selecting an oral contraceptive.
How Do Specific Health Goals Influence Pill Selection?
Your specific goals point to formulations most likely to deliver the desired results. For acne, combined pills with anti‑androgenic progestins are often effective. For heavy periods or endometriosis, extended‑cycle or continuous regimens reduce endometrial growth and bleeding. If you’re breastfeeding or have an estrogen contraindication, progestin‑only options provide contraception without estrogen exposure and with minimal effect on milk supply. When cardiovascular risk is a concern—because of smoking or age—non‑estrogen methods or long‑acting reversible contraception may be safer, so individualized counseling is important.
What Are the Most Frequently Asked Questions About Birth Control Pills?
Below are concise, practical answers to common concerns—missed pills, weight and mood effects, stopping the pill, and interactions—so you can act quickly and know when to seek clinical help. Short, evidence‑based answers help you find reliable guidance and plan follow‑up with your clinician when needed.
What Should You Do If You Miss a Birth Control Pill?
Steps depend on the pill type and how many doses were missed. For combination pills: if you miss one active pill, take it as soon as you remember and continue the pack; if you miss two or more, follow the specific instructions on your pack, use backup contraception, and consider emergency contraception depending on timing and unprotected sex. For progestin‑only pills: a dose taken outside the strict timing window (usually more than 3 hours late) should be taken right away, and you should use condoms for 48 hours; consider emergency contraception if you had unprotected intercourse during the risk window. When unsure, treat the situation as higher risk: use condoms, consult a provider, and consider emergency contraception if appropriate.
Can Birth Control Pills Cause Weight Gain or Mood Changes?
Evidence shows little consistent link between modern birth control pills and significant weight gain for most users, though individual experiences vary and lifestyle factors can play a role. Mood effects are individual: some people note worsened mood or depressive symptoms with certain formulations, while others feel no change or even improvement. Monitor weight and mood during the first few cycles; if changes are meaningful or persistent, talk with your clinician about trying a different progestin, adjusting the formulation, or switching to a non‑hormonal method. Open monitoring and communication help tailor choices to your wellbeing.
Our aim is to give clear, user‑friendly answers about the benefits, risks, and options for birth control pills so you can make informed choices and feel confident discussing options with your healthcare provider.
Conclusion
Knowing the benefits and risks of birth control pills helps you choose a method that fits your health needs and lifestyle. Pills can regulate cycles, ease symptoms, and lower certain long‑term cancer risks, but they also carry side effects and contraindications that require careful consideration. Talk through your personal health goals and risk factors with a healthcare provider to find the right formulation or alternative method. When you’re ready, explore our resources and connect with a clinician to take the next step in your reproductive health journey.